Introduction to Fertility: Gametes, Ovarian Reserve, and Oocyte Quality
Document from University about Introduction to Fertility. The Pdf provides a detailed introduction to human fertility, exploring the formation and characteristics of male and female gametes. The Pdf, suitable for University Biology students, covers topics like ovarian reserve, oocyte quality, and modulating factors such as AMH and FSH, presented with clear explanations and supporting graphics.
See more10 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Introduction to Fertility
Gametes
Both male and female gametes originate from the same stem cells contained within the yolk sac. The yolk sac is visible very early in the transvaginal US scan soon after positivity to pregnancy test, at about 2 weeks of pregnancy, in particular just after appearance of foetal heartbeat. In the US it is possible to visualize the gestational chamber inside the uterus which houses the foetus (about 1 cm within the gestational chamber with heart beating inside it), and, aside from the foetus, a ring which is the yolk sac. In the latter stem cells are present, which will later develop and become gametes. Stem cells actively increase their number and will then migrate through a tube named allantois which connects the yolk sac to the central part of the foetal body. Stem cells become gametes and they localize in a connective tissue close to the kidneys, which are the primary gonads.
Male Gametes
In case of presence of a male chromosome in karyotype there is expression of protein SRY (=expression of Y chromosome) which makes the ring evolve into testicles. Testes are long tubular structures of approximately 2 meters per testicle within a relatively smaller overall volume. Inside the testes, stem cells lay. At birth, the male neonate does not have any spermatozoa. In puberty spermatozoa appear thanks to the signal sent from the hypothalamic-hypophysis-testicular axis promoting stem cells and seminiferous epithelium to mature and differentiate into sperm cells. Once puberty hits, men will continue to produce spermatozoa for the rest of their life. The seminiferous epithelium has got regenerative potential that enables it to continue producing new spermatozoa from stem cells in the testes. As far as quantity is concerned, the number of spermatozoa that is produced keeps on lowering while going on with age; however, as far as quality is concerned, it will be constant throughout life, which is why males can father healthy children even when they are older as spermatozoa are constantly produced in a cycle lasting 3 months. In other words, regardless the age, males always have new and functional spermatozoa that are at most 3 months old. To be precise, there is a slight decrease in quality starting from 50 years of age which implies an increased risk of child having autism or schizophrenia, but all the other diseases including risk of spontaneous abortion and unsuccessful pregnancy are unaltered regardless of father's age.
Female Gametes
In absence of a Y chromosome, SRY protein is not synthesized, thus genital rings organize themselves as ovaries. Ovaries do not have a tubular organization, but they are formed as a cluster, connective tissue organizes itself around a stem cell, aka the oocyte, and it creates a structure known as follicle. Ovaries are full of ovarian follicles. Each one contains an ovum with granulosa cells (highly specialized connective cells) and even more externally thecal cells (once again connective tissue). The follicle is a functional unit where cholesterol comes from blood, thecal cells convert cholesterol into androgens which are in turn converted by granulosa cells into estrogen. In the absence of follicles and its connective tissue cells it is impossible for an ovum to grow and become fertile, as granulosa and thecal cells are necessary to provide the egg with the essential nutrients that allow for its maturation. Removal of follicle around an ovum results in atrophy of the latter. Virginia Gallina, Miriana La Bua 1PROF. REVELLI- L01 Formation of new follicles in female foetus can happen only in the first half of pregnancy. From 25th week of pregnancy, it is impossible to produce any other follicle and it will remain impossible throughout all of patient's life. Females are born with all their oocytes for all their life in the ovaries. There is no regenerative power, stem cells cannot multiply and new oocytes cannot be formed; still nowadays there is no therapy to restore oocytes production in the ovaries.
Ovarian Reserve and Oocyte Quality
Like all tissues in our bodies, ovaries age due to mutagens inducing apoptosis in our cells (we become older because our cells accumulate mutations up to the point of dying or experiencing programmed cell death). Most tissues, such as the skin, have regenerative power and can replace old cells with new cells; however, ovaries do not have such a capacity. When follicles go into apoptosis the oocyte inside is permanently lost and cannot be replaced; eggs are continuously lost from the 25th week of foetal life onwards. The ovarian reserve is defined as the total amount follicles contained in both ovaries. It is maximal before birth. Women decrease their ovarian reserve by 1000 follicles a month (slides: 500-800 follicles) due to the physiological process of becoming older. These follicles are going to be lost anyway, even when taking the pill, during pregnancy and lactation. It is not stoppable because it is due to an FSH-independent physiological apoptotic phenomenon related to aging which is present in all tissues. Follicular loss does not follow a linear pathway, it becomes more and more rapid after age 25. This curve shape is likely due to the reduction of intraovarian factors modulating follicular activation and counteracting apoptosis. When there are only approximately 1000 follicles left, they cannot sustain the endocrine requirements necessary for menstruation, thus menopause occurs. There is thus a decrease in the quantity. There is indeed a change in quality as well. Quality of the oocyte is defined as its competence to undergo fertilization and sustain embryo development. It is the result of:
- Genetic asset (23X)
- Structure and function of subcellular organelles
- Metabolism
- Biochemical pathways.
Meiosis1 is the evolution from somatic cells to gametes which carry only half of the genetic makeup (23 chromosomes instead of 46). In males meiosis is a continuous phenomenon which starts with the duplication of DNA (from 2n to 4n, then first meiotic division into 2n + 2n and finally second meiotic division into 1n + 1n + 1n + 1n, thus from one stem cells 4 spermatozoa are generated). During the meiotic process, DNA is possibly susceptible to mutagens as it is not protected by histones; however, once started, meiosis in males is completed in a matter of a few days, therefore allowing the male gamete to be exposed to and wounded by mutagenic agents only for a very limited amount of time. Indeed, it is rare for sperm DNA to be mutated. As they are built very quickly, they may be morphologically abnormal with fragmented DNA (millions are produced but only a percentage is morphologically normal), however, there is no mutagenesis. 1 Whereas mitosis is exclusively the multiplication of cells. 2PROF. REVELLI- L01 In females, the ovarian meiosis starts when the female foetus is not born yet and it stops in prophase (first phase, particularly in diplotene substage) of first meiotic division. DNA remains duplicated in the cells for years, therefore being exposed to mutagenesis. In puberty, meiosis starts again; each month with ovulation the first meiotic division of that single egg is completed. The second meiotic division then starts but it stops again in metaphase in the salpinx. Only fertilized eggs will then complete the second meiotic division, as the factors to proceed with meiosis are supplied by the spermatozoon entering the oocyte. All other oocytes do not finish meiosis. Any mutation can occur in the duplicated DNA in those years in which meiosis is stopped (once again, duplicated DNA is not protected by histones). Sometimes the mutation is meaningless, causing minimal damage or it may be repaired. However, other times, mutations can induce damage which cannot be fixed. This situation worsens year after year with aging, as mutations accumulate and the quality of eggs decrease. Going on with age, not only the number of eggs diminishes, but so does the proportion of normal eggs out of the total. Only a normal egg can grow into a healthy baby. Only a normal egg can be fertilized, become an embryo, implant into the endometrium and pregnancy can proceed with no abortion, no foetal death and no foetal diseases.
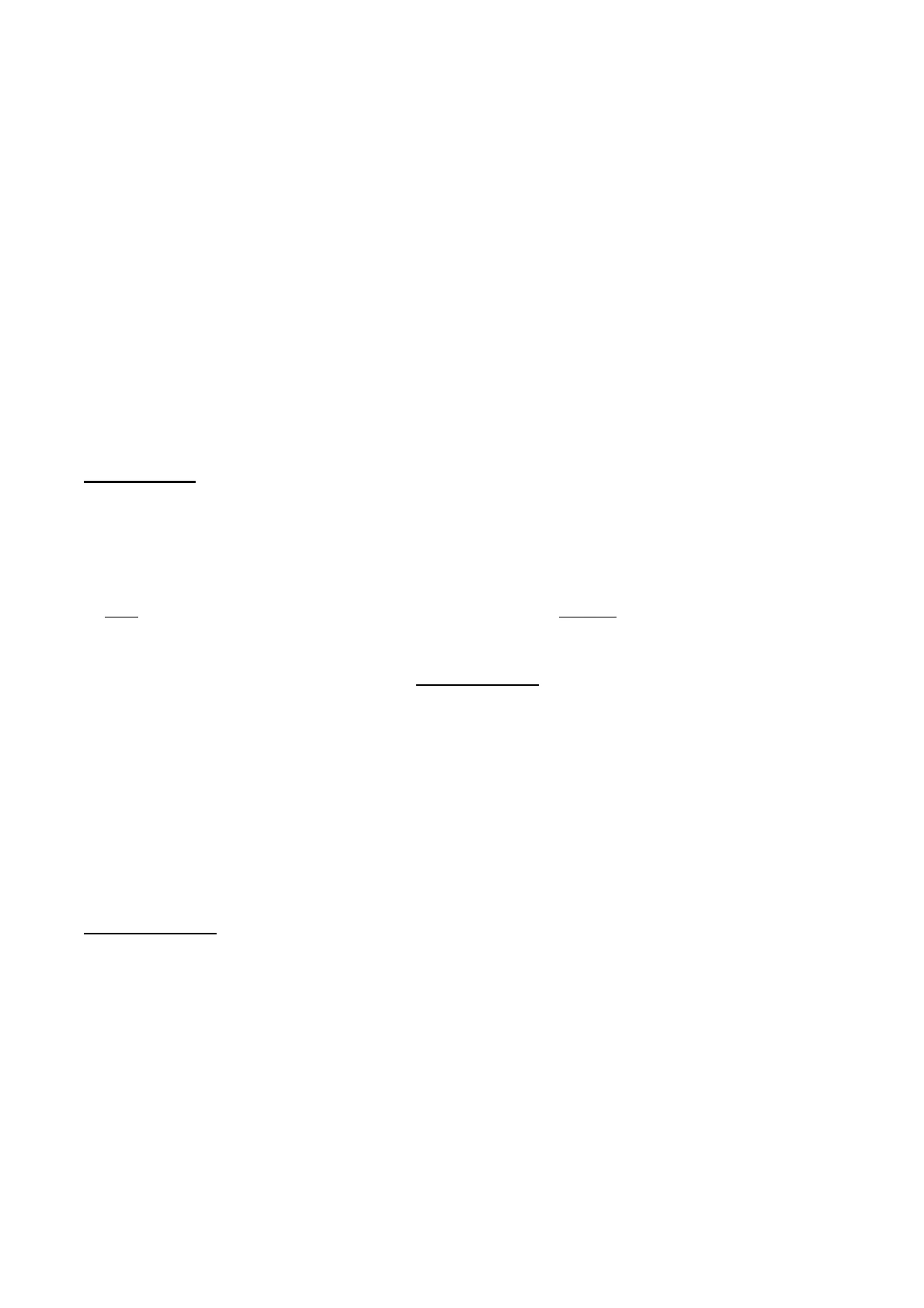
Probability of Live Birth by Age
100 Probability of having at least one live birth 90 80 70 60 50 Age (y) 40 Donor 30 37 20 42 10 43 44 0 0 10 20 30 40 50 60 70 BD 90 100 Number of mature oocytes
- At 20 years old: 1 egg out of 3 is normal
- Between 25 and 37 years old: 1 egg out of 5 is normal
- Between 38 and 39 years old: 1 egg out of 7 is normal
- At 40 years old: 1 egg out of 9 is normal
- At 41 years old: 1 egg out of 14 is normal
- At 42 years old: 1 egg out of 20 is normal
- At 43 years old: 1 egg out of 35 is normal
- At 44 years old: 1 egg out of 55 is normal
- At 45 years old: 1 egg out of 85 is normal
For instance, at 41 years old, as you ovulate 12 times a year, only less than one of these ovulations has probability to become a healthy baby. Oocyte genetic and structural quality worsens with age due to the following reasons:
- All oocytes available throughout life are already contained in the ovaries at birth. Woman's age = age of her eggs;
- The ovulated oocyte every given month has the same age of the woman; 3PROF. REVELLI- L01
- Oocytes enter the first meiotic division during foetal life, but meiosis stops at a very early stage (prophase of the I meiotic division), when DNA is duplicated and is not bound to histones (despiralized chromatin);
- This "helpless" DNA is exposed to be damaged by environmental factors (mutagens, oxidants, etc.);
- Damages of the DNA accumulate and may cause oocyte death (apoptosis);
- If the oocyte survives, DNA damage is there when that oocyte is ovulated and eventually may be transmitted to the embryo;
- The same is true for damages of mitochondrial DNA or of other organelles.
Female Fertility Decline
Proportion of euploid embryos 500- Fertility -100 450- -90 Fertility Rate (per 1000 married women) 400- -80 350- -70 300- -60 250- -50 200- -40 150 30 Spontaneous 100 20 abortions 50- -10 O 20 24 25-29 30-34 35-39 40 44 =45 Maternal Age (yr) Maternal Age {yr) Demko et al., 2016
- Female fertility declines as a result of reduced fecundity plus increased abortion rate, both due to worse genetical/structural oocyte quality
The number of oocytes needed to get a live birth increases with age. As shown in the graph below, at 36y to have 60% of chance to become a mother, 10 oocytes are needed thus 1y of ovulation, at 43y to have the same probability, 64 ovulations are needed which is roughly 5y, but 5y in a woman which is already 43y are too much, so there will never be a 60% chance. Taking into account both the quantity decrease in the ovarian reserve and the quality decrease of oocytes, it sorts out that epidemiologically it is a sporadic event to get pregnant with a healthy baby after the age of 44 years. THE AGE LIMIT TO CONCEIVE AND HAVE A HEALTHY BABY FOR A WHITE CAUCASIAN WOMAN IS 44 YEARS. After that it is not impossible, but it is a sporadic event; it is so low that there is no way to establish an epidemiological percentage of pregnant women beyond that age. (of course, it is different when dealing with donors). The quality of the egg can only be predicted by looking at the quality of the embryo and foetus. This age limit depends on ethnicity. In Asian women it is 42.5 years, as they present anticipated menopause, whereas Latin American women it is 45.5 years. African is the same as White Caucasian. This is the maximum limit, not an average. There may be individual variation which tends to anticipate age limit for healthy conception and pregnancy. Not only genetic variance (for mother hitting menopause precociously could mean constitutional predisposition to early menopause) but also acquired diseases in the ovaries such as benign teratomas, cysts or endometriosis affect the age limit. The ill component of the ovary loses follicles, thus causing an increased velocity of oocyte loss. It also happens in case of chemotherapies for other reasons, which implies the loss of some of the eggs. In case of radiotherapy in pelvis or total body irradiation (such as for bone marrow transplant) Rate of Spontaneous Abortions (%) Percentage Euploid 31 60- 10 (mean ± SD) 13 15 20 25 30 35 40 45 150 4
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
