Stroke: Definition, Epidemiology, Risk Factors, and Treatment Strategies
Slides from Jessica Teng Margherita Marotta Vascular Surgery - Stilo about Stroke. The Pdf provides a detailed overview of stroke, including its definition, epidemiology, risk factors, and related steno-obstructive diseases. It also discusses cerebral vascular anatomy, particularly the circle of Willis, and treatment strategies like carotid endarterectomy.
See more12 Pages

Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Jessica Teng Margherita Marotta
Vascular Surgery - Stilo 27.03.2025
Stroke
Epiaortic diseases
-definition- Neurological ischemic problems due to reduced hematic flow to the brain
STROKE
- A stroke occurs when the blood supply to pan or your brain is interrupted or reduced, preventing brain tissue from getting oxygen and nutrients. Brain cells begin to die in minutes.
- A stroke is a medical emergency, and prompt treatment is crucial. Early action can reduce brain damage and other complications.
Steno-obstruct diseases
Now we can start to study steno-obstruct disease. For example, the same atherosclerotic plaque could cause ischemia in our organs (kidneys, limbs).
Stroke Ischemia
In the case of ischemia at the level of the brain, we have ischemia that is called stroke. It's an ischemic problem due to reduced hematic flow at the level of the brain. Our brain is an important organ, presenting a lot of collateral circuits at the level of Willis polygon. It's an important cause of death, an important pathology for people more than 55 years old. 50% of strokes are due to carotid disease.
Stroke Epidemiology
-epidemiology-
- 3 cause of death
- 1 cause of disability
- People age 55 or older have a higher risk of stroke than do younger people
- 50% of stroke due to carotid diseases
Stroke Risk Factors
Many factors can increase your stroke risk. Potentially treatable stroke risk factors include
- Being overweight or obese
- Physical inactivity
"Heavy or binge drinking
- Use of ilegal drugs such as cocaine and methamphetamine
- High blood pressure
-Cigarette smoking or secondhand smoke exposure -High cholesterol -Diabetes Obstructive sleep apnea
- Cardiovascular disease, including heart failure, heart defects, heart infection or abnormal heart rhythm, such as astal fibnltation
-Personal or family history of stroke, heart attack or transient ischemic attack -COVID-19 infection Other factors associated with a higher risk of stroke include:
-Age -- People age 55 or older have a higher risk of strolus than do younger people. -Race -- African Americans have a higher nsk of stroke than do people of other races -Sex- Men have a higher risk of stroke than women. Women are usually older when they have strokes, and they're more likely to die of strokes than are men
- Hormones - Use of birth control pils or hormone therapies that includes estrogen increases risk
Risk Factors for Atherosclerotic Pathology
Risks factors are the same for all atherosclerotic pathology:
White and red
- smokers
- Diabetes
- And so on
Other factors include:
- Age
- Raceposterior cerebral arteries Internal Carotid artery Carotid bifurcation External Carotid artery anterior communicant artery Common Carotid artery internal carotid artery external carotid artery 6th cervical vertebra vertebral artery ELST subclavian artery Superficial temporal artary -Middle meningenl srtary Supratrochlear artery . Supraorbital- artery Anterior cerebral artery Middie Coraliei artery postarter communicating artery Angular artery. Ophthalmic artery Posterior Escalival AsEller artery Internal maxillary artery Internal carotid artery Occipital artery Facial artery -Vertebral artery External carotid artery Common carotid artery
Anatomy of Aortic Vessels
Anatomy: When we talk about the aortic vessel, we talk about the:
-
Carotid artery: the carotid artery is responsible for the anterior circulation of the brain.
o Right carotid artery is born from the innominate artery o Subclavian carotid artery is born directly from the aortic arch o Neck level: we have no collateral circle, so we only have the common carotid artery
➢ Internal carotid artery didn't have collaterals
➢ External carotid artery has some collateral arteries
- Between external and internal carotid arteries, we have a lot of collaterals at the level of the ophthalmic artery, with internal maxillary artery, and we also have other anatomical collateralization
- Vertebral artery: vertebral artery is responsible of the posterior circulation of the brain. At the level of the base of the skull, we have the Willis polygon. So, we have the communication between the anterior and posterior circle.
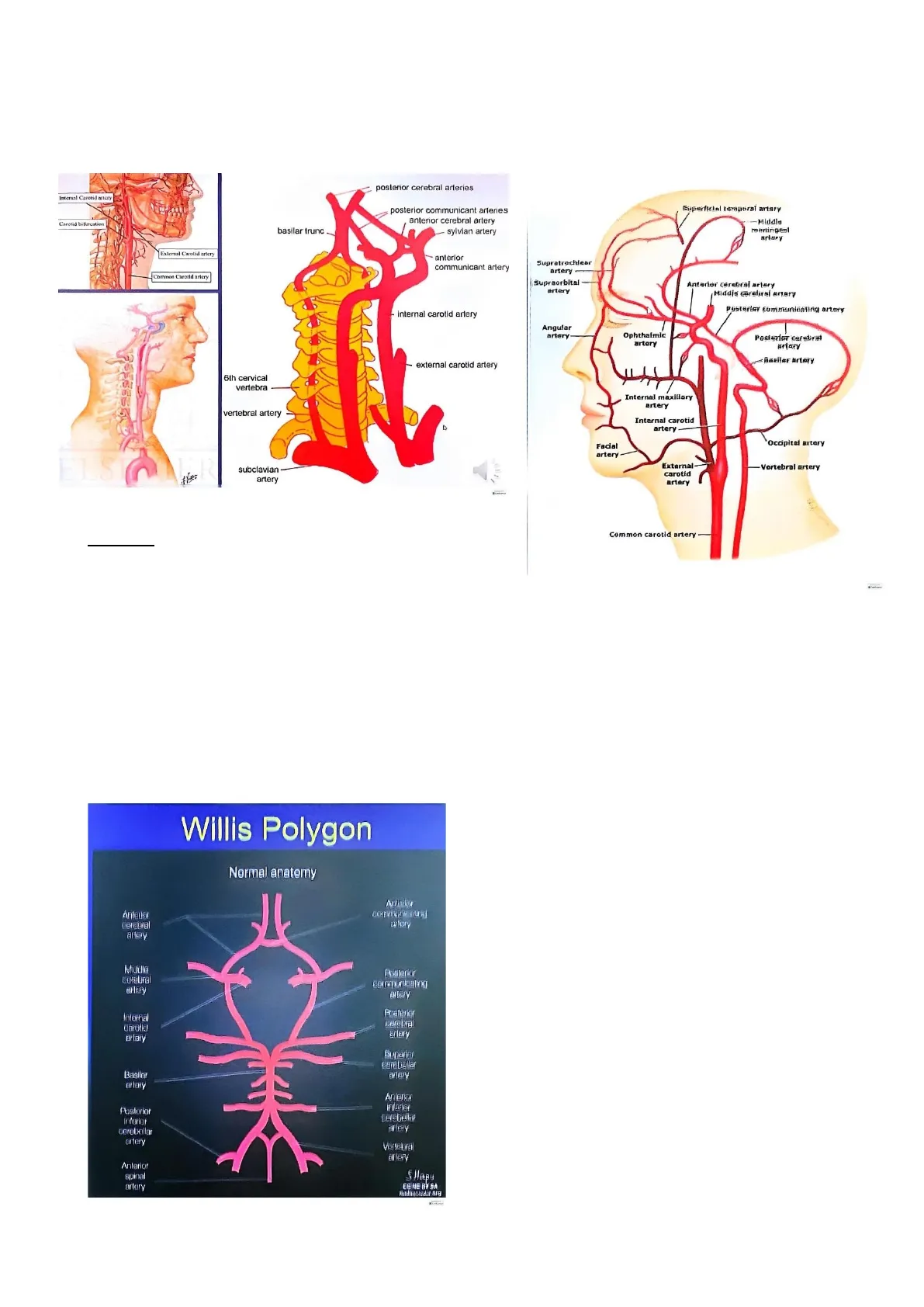
Willis Polygon Normal Anatomy
Normal anatomy Åntener aftery Middle combral Eftery Posterior Internal carotid Ertery artery Buparjer cerebellar AFLerY Basilar artery Antener interior Cerabella artery Posterior Inferior corobollar artery Vertebral Eftery Anterior spina artory SHapu CE NE BY SA We have an important collateral communication between anterior and posterior circles. This is important when you have an ischemia because we have to know if the ischemia is at either the anterior level or posterior level. We have different symptoms in the left brain, right brain, or posterior region.
posterior communicant arteries anterior cerebral artery sylvian artery basilar trunc
Stroke Causes
Causes: The principal causes of stroke are 30% carotid diseases. However, a lot of strokes are due to small and large vessels atheroembolism, diabetes, and cardioembolism. Thus, the first causes of stroke include:
- Atrial fibrillation
. Atheroembolism from the arch atrial
- Atheroembolism from carotid disease. In the case of carotid disease, we have problems due, not only to the obstruction rate of stenosis, to the fact that part of the plaque goes to the brain. So, you carry an embolism from the carotid source. Instead, in case of coronary disease, the problem is due to an obstructive rate of stenosis.
Ischemic Stroke Causes
CAUSE DICTATES MANAGEMENT
LARGE VESSEL ATHEROEMBOLISM (most common)
- Artery to artery embolism
- Thrombosis in situ
SMALL VESSEL ATHEROEMBOLISM
- Lacunar disease associated with hypertension and diabetes
LOW-FLOW STATE
- Ischemic "watershed" areas
CARDIOEMBOLISM
- Nonvalvular AF
- Post-MI
- Dilated cardiomyopathy
- Prosthetic heart valves
- Rheumatic heart disease
- Infective endocarditis
- Patent foramen ovale
Stroke Symptoms
Symptoms: When you talk about symptoms, we have TIA (transfer ischemia attack). It's an attack leading to an ischemia at the level of the brain, but this ischemia didn't remain after 24 hours (transitory attack) and we didn't detect ischemia level MRI Symptoms depend on the left side and right side. For example, we have symptoms like troubles in speaking and understanding, and paralysis of the face, arm, or leg. If you have a problem at the level of the left brain, we have a problem of the level of the right limb. The left brain also presents troubles in speaking, because we are in case of a problem affecting the Rolando circle. This will lead to aphasia, because it's impossible to speak and to understand. There may also be problems at the level of the facial nerves, like ptosis.
- TIA secondary to significant carotid artery stenosis -> ~ 30-40% risk of stroke within the next 5 years
- In symptomatic patients, 2-year risk - 22% with 50%-69% (moderate) stenosis vs. 26% in 70% - 99% (severe) stenosis
- In asymptomatic patients, 5-year risk - 7.8% with <50% stenosis vs. 18.5% in 75% - 95% stenosis
Circulation 2006,1 13 e873-923
Transient Ischemic Attack (TIA)
A transient ischemic attack (TIA) - sometimes known as a ministroke - is a temporary period of symptoms similar to you'd have in a stroke A TIA doesn't cause permanent damage. They're caused by a temporary decrease in blood supply to part of your brain, which may last as little as five minutes. Like an ischemic stroke, a TIA occurs when a clot or debris reduces or blocks blood flow to part of your nervous system Seek emergency care even if you think you've had a TIA because your symptoms got better It's not possible to tell If you're having a stroke or TIA based only on your symptoms. If you've had a TIA, it means you may have a partially blocked or narrowed artery leading to your brain. Having a TIA Increases your risk of having a full-blown stroke later.
- Trouble speaking and understanding what others are saying. You may experience confusion, slur your words or have difficulty understanding speech.
- Paralysis or numbness of the face, arm or leg. You may develop sudden numbness, weakness or paralysis in your face, arm or leg. This often affects just one side of your body. Try to raise both your arms over your head at the same time. If one arm begins to fall, you may be having a stroke. Also, one side of your mouth may droop when you try to smile.
- Problems seeing in one or both eyes. You may suddenly have blurred or blackened vision in one or both eyes, or you may see double.
- Headache. A sudden, severe headache, which may be accompanied by vomiting, dizziness or altered consciousness, may indicate that you're having a stroke.
- Trouble walking. You may stumble or lose your balance. You may also have sudden dizziness or a loss of coordination.
Carotid Plaque Evolution
Carotid's plaque
Foam cells Fatty streak Intermediate lesion Atheroma Fibrous plaque Complicated : lesion/rupture 1 2 3 4 5 Decade Growth mainly by lipid accumulation Smooth muscle Thrombosis. hematoma and collagen The most important thing at the level of carotid vessels is related to carotid disease, because it's the most popular carotid problem than vertebral problem or problem at the level of aortic arch. So, we have a typical atherosclerotic plaque. This plaque grows at level of the carotid bifurcation. There is a plaque initially at the level of the intima, inflammation, growth of the plaque, and so on.
Physiopathologic Mechanisms of Plaque Formation
Physiopathologic mechanisms The problem at the level of the brain is fundamentally embolic and associated to a hemodynamic problem when we have ischemia. Why are the plaques forming at level carotid bifurcation? Why are our plaques forming always at the level of the bifurcation (heart, limbs)? Because when you have a bifurcation, the flow at the level of the bifurcation is not a laminar flow but naturally it's a turbulent flow. In case of the growth of the plaque, this turbulence has increased further favoring the growth. At the level of carotid bifurcation, we have two different flows because there are two different resistances at the level of the internal and external carotid arteries:
High struss Low ponphoral uststane
- Localization: - Carotid bifurcation
Cross. section
- Composition: - lipidic - calcified
- Complications: - Subintimal hemorrhage carotid occlusion Acute thrombosis intimal lesion Į ulceration -> cerebral embolization =
- The internal carotid has low resistance, because the flow at the level of the brain, as at the level of the heart, is a continuous flow (diastolic flow). - Differently, at the level of the external carotid artery (muscular artery) we have a tri-modal flow. Thus, the turbulence at this level is more common. Plaques can be:
- Lipidic plaque: more unstable
- Calcified plaque: more stable plaque. This depends on when the plaque grows. If you have a calcification of the plaque, it will remain with 9%of cholesterol inside of the plaque, so we have an unstable plaque. It's important also to consider the surface of the plaque. If the surface is a good surface or is non-frustrous surface. In the latter, the plaque is more unstable. To have an embolism, we need two factors:
. An important plaque with a stenosis rate of more than 17-18%
- Unstable surface We also need stenosis because we need an acceleration of the flow at the level of the stenosis.
Endothelial dysfunction
A
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
