The Gastrointestinal System: Dyspepsia, GORD, and H. pylori
Slides from University about The Gastrointestinal System. The Pdf explores the gastrointestinal system, analyzing potential causes of dyspepsia, oesophagitis, gastritis, peptic ulcers, GORD, and Helicobacter pylori infection. This University Biology presentation, produced for university students, also covers NSAID-induced gastropathy.
See more26 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Dyspepsia and Upper GI Disorders
Potential Causes of Dyspepsia
Dyspepsia A non specific term, encompasses a number of symptoms attributable to the upper GI tract. Oesophagitis Gastro oesophageal reflux disease (GORD) Barrett's oesophagus Gastritis Type A Type B Type C Peptic ulcers Gastric ulcer Duodenal ulcer Zollinger-Ellison Syndrome Gastric cancer.
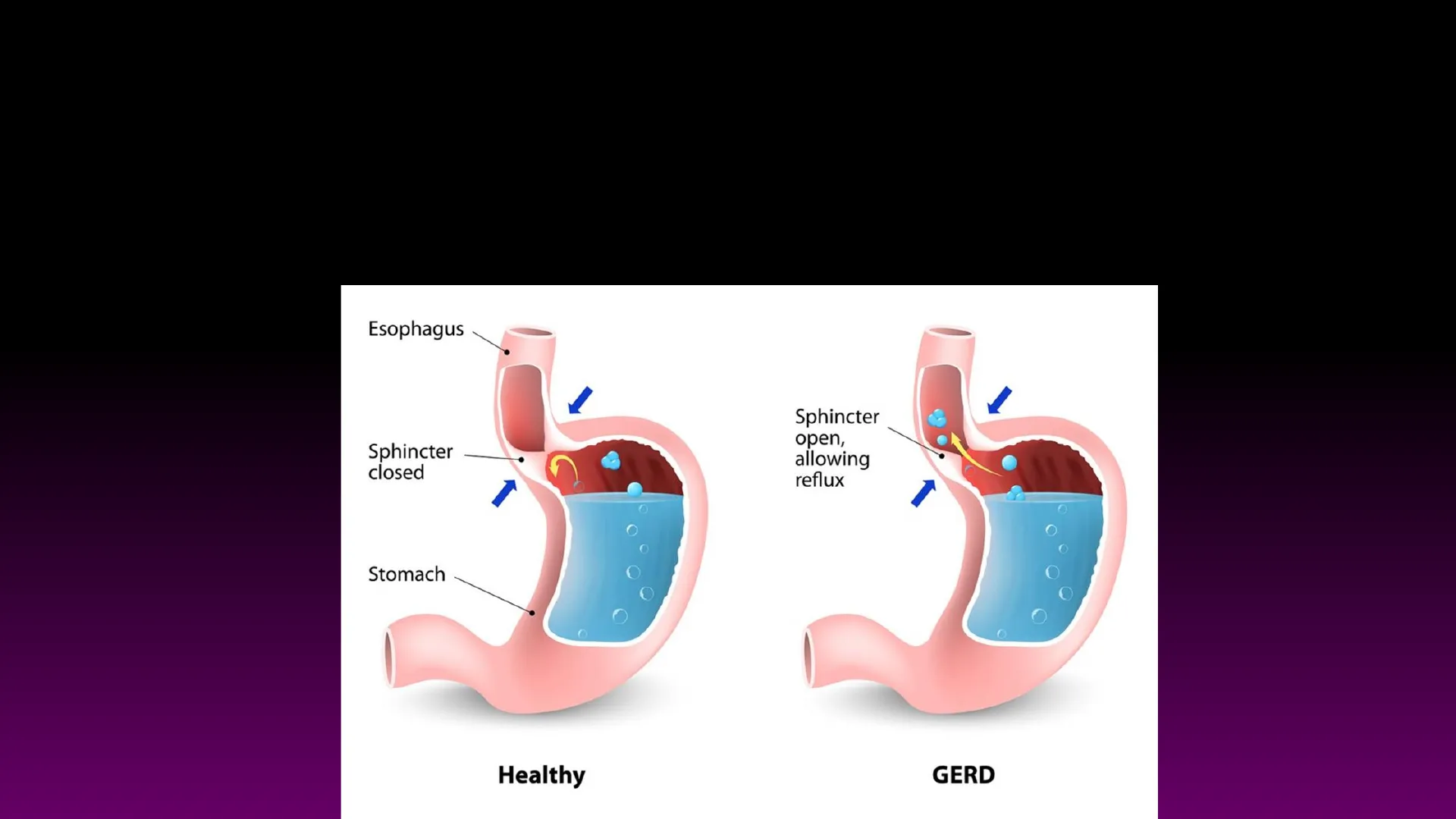
GORD and Oesophagitis
GORD or GERD Esophagus Sphincter closed Sphincter open, allowing reflux Stomach O Healthy GERD 2The Oesophagus . The mucosa of the oesophagus is . non-keratinzed stratified squamous epithelium . The type of muscle in the muscularis of the oesophagus varies by region ◦ the superior 1/3 is skeletal muscle ◦ the intermediate 1/3 is skeletal and smooth muscle the inferior 1/3 is smooth muscle ◦ ◦ Adventitia replaces serosa. non keratinized stratified squamous epithelium Lumen of esophagus Mucosa: Nonkeratinized stratified squamous epithelium Lamina propria Muscularis mucosae Submucosa Muscularis (circular layer) Muscularis (longitudinal layer) Adventitia LM 20x (a) Wall of the esophagus Copyright @ John Wiley & Sons, Inc. All rights reserved.
Barrett's Oesophagus
oEndoscope Normal squamous esophagus Top of hiatal hernia (normal stomach folds) -Squamocolumnar junction "Tongues" of Barrett's Barrett's esophagus Diaphragm Stomach Actual endoscopic photo Photo courtesy of the Seattle Barrett's Esophagus Research Program Long-standing reflux of acid About 1 in 10 people with GORD develop Barrett's oesophagus. Normal stratified squamous epithelium is replaced with simple columnar epithelium with goblet (mucus cells).
Techniques to Improve Diagnosis of Barrett's Oesophagus
NAME: A B Figure 5: Oesophagus: A: routine endoscopic appearances. B: post acetic acid chromoendoscopy (Obtained using an Olympus standard definition gastroscope) If left untreated! NORMAL, HEALTHY ESOPHAGUS ESOPHAGUS DAMAGED BY PROLONGED ACID EXPOSURE BARRETT'S ESOPHAGUS TISSUE DYSPLASTIC BARRETT'S ESOPHAGUS ESOPHAGEAL CANCER Disease progression NAME:
Control and Regulation of Acid Secretion
Gastric Mucosa Blood Flow and Parietal Cells
Gastric Mucosa Blood Flow Carrier Proteins (transporters) in parietal cells Acid flow rk Surface mucous cells Mucous = coating Luminal 'acids Lumen Interstitial space H+ H2O Na+ - · CI- Fenestrated capillary Muscularis Mucosa 2 K+ HCI Parietal cell ATP Bicarbonate flux Submucosa Chief cells Parietal cells Mucous cells H+ ATP OH- CI- CA CO2 CO2 Endocrine cells Blood flow Submucosal venule Submucosal arterioles Proposed Vascular Transfer of HCO3 The formation of bicarbonate ions through the activity of carbonic anhydrase is an important barrier to auto digestion and denaturation by H+ ions. Blood flow in the capillaries within the gastric gland runs from the base of the gland to the surface epithelium (blue line) and this allows bicarbonate ions to be secreted across the surface epithelium, resulting in the formation of a protective buffering layer of bicarbonate beneath the layer of gastric mucus. Adequate blood flow is essential to maintain this layer of buffer and this is maintained by the eicosanoid vasodilator, prostaglandin E2 (PGE2). Drugs which interfere with the production of PGE2 such as NSAIDS (e.g. aspirin, ibuprofen) and SAIDS (eg. prednisolone), can cause gastric ulceration. Copyright 2002, Elsevier Science (USA). All rights reserved. Gastric pit Protective bicarbonate flux Gastric Mucosa JAC low 3 Na+ K+ K+ HCO3 HCO3 Mucosal venule H2O Mucosal capillaries
Receptors Stimulating and Inhibiting Acid Secretion
Receptors The receptors involved in stimulating acid secretion are outlined in RED and thise receptors which inhibit acid secretion are outlined in GREEN. CCKB Gastrin . This slide summarises the control of acid secretion and also describes the cell signalling pathways involved for each receptor. Abbreviations: PIP2 (Phosphatidylinnositol-4,5-phosphate), PLC (Phospholipase C). Gq (phospholipase linked GTP binding protein), IP3 (inositol-1,4,5-triphosphate)., DAG (di-acyl-glycerol), PKC (protein kinase C), ER (endoplasmic reticulum) Gs (Adenylate cyclase stimulating GTP-binding protein), Gi (Adenylate cyclase inhibiting GTP-binding protein), AC (adeylate cyclase), PDE (phosphodiesterase), PKA (protein kinase A) CCKB Gastrin PIP 2 M3 receptor Ga DAG > K+ Ca2+ H2 Histamine H+ PKA Gs H-K pump CAMP Somatostatin receptor Parietal cell AC ATP TCAMP Somatostatin receptor AC ATP Gi Somatostatin Gi Somatostatin Prosta- glandin receptor Prostaglandins PIP2 M3 receptor DAG PLC Y PKC IP3 Lumen of antrum PLC · ACh PKC IP3 Ca2+ Ca2+ H2 Histamine 5'AMR H+ İPKA . Gs PDE TH-K pump Parietal cell Prosta- glandin receptor Prostaglandins Lumen of antrum K+ ER . ER 4Ca2+ · ACh Ga
Acid Secretion Summary
- M3 and CCK2 (CCKB; gastrin) receptors - GTP-binding protein coupled receptor (GPCR) - Linked to Gq (stimulates Phospholipase C) - Increases intracellular Ca2+ via PIP2 conversion to DAG & IP3
- H2 receptors - GTP-binding protein coupled receptor (GPCR) - Linked to Gs (stimulates adenylate cyclase) - Increases intracellular cAMP
Treatments for Dyspepsia
Dyspepsia Treatment Evolution
- Surgery (1900-1970's) - Gastric vagotomy & antacids
- Drugs (1970's onwards) - Barriers/protection · Alginate · Sucralfate- antacid & barrier - Muscarinic cholinergic receptor antagonists (M3) · Pirenzepine - Selective H2 receptor antagonists · Cimetidine, ranitidine, famotidine.
- Drugs (1990's onwards) - Proton Pump Inhibitors · Omeprazole, pantoprazole, lansoprazole, rabeprazole & esomeprazole
Relon Chem ranitidine75. Rennie PEPPERMINT GAVISCON GAVISCONSST2R G cell 1 Gastrin Proglumide AA CCK2R PGE2 Somatostatin SST2R ECL cell EP2/3R NSAIDS 1 Misoprostol Histamine H2R H2 blockers SST2R CCK2R? M3R - Ach PARIETAL CELL H+ K+ CI 1 1 1 1 1 P c 1 1 1 1 1 H+ K+ CI
Control of Gastric Acid Secretion
- Items in green inhibit or reduce acid secretion.
This is the three cell system for the control of acid secretion with gastrin being released from the gastric G- cell and histamine being released from the ECL (enterochromaffin like cell; which is the equivalent of a mast cell). The receptors include the SST2R (somatostatin type 2 receptor), CCK2R (cholecystokinin type 2 receptor which responds to gastrin), the H2 (histamine type 2 receptor) and the M3R (muscarinic cholinergic type 3 receptor). Proton pump inhibitors Atropine
Chemical Structure of Losec and PPIs
OCH, HỌC CH, OCH Lasec Pharmacist Only Medicine Losec Omeprazole 10mg 24-Hour Relief from Heartbom & Acid Reflux Losec Chemical name: (RS)-5-methoxy-2-[[(4-methoxy-3,5-dimethyl- 2-pyridinyl) methyl]sulfinyl]-1H- benzimidazole Proprietary name: Losec Generic Name: omeprazole Other examples of drugs belonging to PPI class of drugs. Pantoprazole, Lansoprazole, Esomeprazole, Rabeprazole, Relieves Heartburn NOVARTIS NEW! 24HR PREVACID Nexium compresse gastroresistenti A028005 esomeprazolo 20 20 mg gastro-resistant tablets Pantoprazole 7 uso orale JANSSEN-CILAG 28 Pariet 20 mg Pantoloc CONTROL® www.buckadaypharmacy.com Losec and other PPI's form an irreversible covalent bond between the drug and the target protein, the proton pump or hydrogen potassium ATP-ase). It is important to note that very few drugs form irreversible covalent bonds, most work through electrostatic interactions with the target protein. Another example of a drug that works through formation of a covalent bond is aspirin which binds irreversibly with the enzyme cyclo-oxygenase (COX).ATP 1033 3 Cytosol X LX VIII VIL VI V IV Apical Membrane Lumen CYS 813 W'ite CHO CHO. S CHO C 1 H S = H. S 0 B
Mucosa Aggressors and Protectors
Mucosa aggressors & protectors CHOLINERGIC NERVE BLOOD VESSEL MR 'MC' GR + ACh Histamine Gastrin AA + HOR MR GR + ECL Cell + PARIETAL CELL Ach Neuron Multiple Cells Ach Multiple Cells Neuron M H PGE 1 1 1 1 1 1 + P C Ca2 -CAMP 1 Blood CCK (+CCKA NO LOGMP- Kinases Mucous Cell MUCUS Aggressive Protective M PGE, H K+ CI 1 1 CAMP Blood CCK (CCKA NO CGMP- Kinases Chief H+ K+ CI Cell Pepsinogen I PGE2 PGR 1
What Causes Dyspepsia?
Protective Mucus Prostaglandins Bicarbonate Mucosal blood flow Aggressive Acid Pepsin NSAID's Helicobacter pylori Drugs Diet
Gastritis
Aetiology and Diagnosis of Gastritis
- Three categories
- Type A = Autoimmune - (antibodies against parietal cells) · Reduced or no acid secretion and intrinsic factor. · Aplastic anaemia due to Vit B12 deficiency
- Type B = Bacterial - Helicobacter pylori infection · Elevated acid secretion
- Type C = Chemical - Chemicals/drugs eg aspirin · Elevated acid secretion
- Pharmacy cohort more details in workshop. 13
Type A Gastritis
- Autoimmune atrophic gastritis
- Destruction of parietal cells - Reduced or absent acid secretion. - Vitamin B12 deficiency. - Anaemia
- Other conditions associated with Type A Gastritis: - Autoimmune thyroiditis (Hashimoto's disease) - Type I Diabetes - Addison's Disease (Adrenal glands, reduced cortisol & aldosterone) - Vitiligo (skin pigmentation disorder) white patches of skin.
- Hydroxocobalamin injections 14
Type B Gastritis: Helicobacter Pylori
Helicobacter pylori
- Associated with: · 80% of gastric ulcers · 95-100% of duodenal ulcers · 100% chronic antral gastritis · gastric cancer (younger infected, greater chance) - Gram negative spiral bacterium, · colonises mucus in both stomach and duodenum. - Secretes · urea from high urease activity (antral pH raised, gastrin & acid secretion increases), · PAF (platelet activating factor),Helicobacter pylori · Gram negative · Doesn't retain Crystal violet stain! stress doesn't cause ulcers - 100! helicobacter pylori Gastric lumen Gastric mucus 3 4 a Motility C Pedestal formation 5 b Adherence d Vac A urease Vacuolization and cell damage Gastric epithelium Inflammation (gastritis) 1 e Infiltration of lamina propria NFKB activation IL-8 secretion Neutrophil 3 Macrophage pH gradient <2 6-7
Eradication of H. Pylori
First Line Treatment (One Week, Twice Daily)
- Amoxycillin 300mg and either · Clarithromycin 500 mg or Metronidazole 400 mg and either · omeprazole 20 mg or lansoprazole 30 mg - Consider lowest acquisition costs and previous exposure to clarithromycin or metronidazole!
If Allergic to Penicillin (One Week, Twice Daily)
- Clarithromycin 500 mg
- Metronidazole 400 mg and either · Omeprazole 20 mg or lansoprazole 30 mg
If Allergic to Penicillin and Previous Exposure to Clarithromycin and Metronidazole (One Week, Twice Daily)
- Tetracycline 1g and metronidazole 400 mg
- Bismuth subsalicylate and omeprazole 20 mg
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
