Anaesthetics: Definition, Mechanisms of Action, and Objectives
Slides about Anaesthetics. The Pdf provides a comprehensive overview of anaesthetics, detailing their definition, mechanisms of action, and the objectives of anaesthesia. This university-level Biology document, produced by an unknown author, explains the differences between general and local anaesthesia, focusing on synaptic and conduction blocks, and includes diagrams illustrating their impact on ion channels.
See more20 Pages

Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Anaesthetics Overview
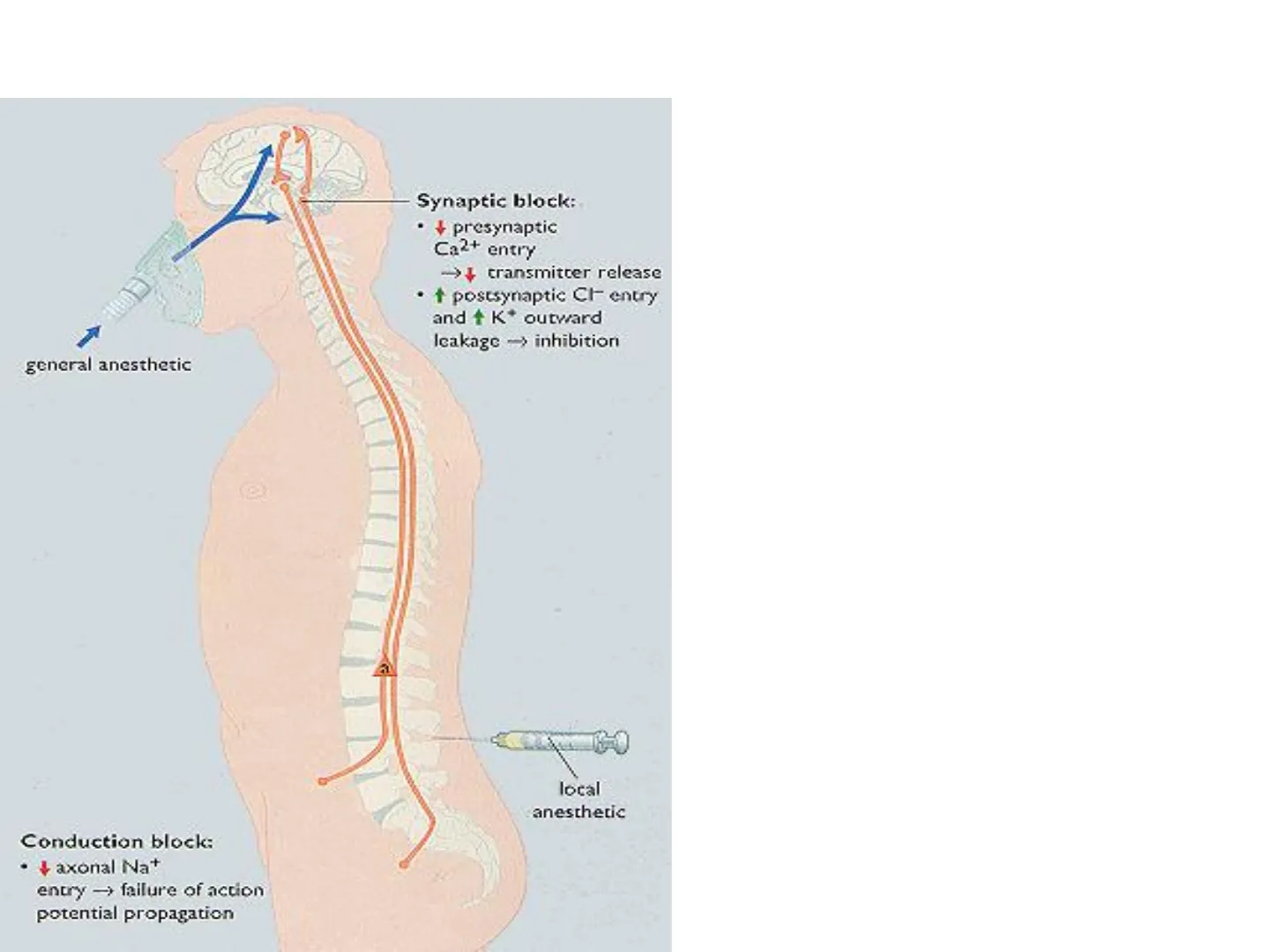
Anaesthetics
Synaptic Block Mechanisms
Synaptic block: · + presynaptic Ca2+ entry ->+ transmitter release · + postsynaptic CI- entry and + K+ outward Icakage -> inhibition general anesthetic
Conduction Block Mechanisms
Conduction block: · + axonal Na+ entry -> failure of action potential propagation local anesthetic
Learning Outcomes for Anaesthesia
- Describe the objectives of anaesthesia.
- Describe the current theories of the Mechanisms of Action of anaesthetics.
- For General Anaesthesia, list the classes of drugs used as Pre-anaesthetic medication and explain the Therapeutic Rationale for their use.
- Describe the different classes of general and local anaesthetics and the reasons for their use.
Definition of Anaesthesia
- Anaesthesia blocking or removal of sensation . Can be provided Locally or Generally
General Anaesthetics: Ideal Agents
General Anaesthetics Ideal agents provide: ➢ a temporary loss of conciousness/sensation ➢ analgesia ➢ muscle relaxation
Mechanisms of Action of Anaesthetics
- Difficulty in determining MOA: => Complexity of anaesthetic state (amnesia, unconsciousness, analgesia and immobility >Multiple organ systems > Diverse side effects e.g. Cardiac; respiratory > Animal models
Mechanisms of Action of General Anaesthetics
- The predominant effect is on SYNAPTIC TRANSMISSION, rather than action potential propogation >> Excitatory synaptic transmission: Anaesthetic are thought to block excitatory receptors such as Glutamatergic; Cholinergic and Serotonergic (5HT) >> Inhibitory synaptic transmission: Generally enhance the function of inhibitory synaptic receptors such as GABA-A receptors; TREK potassium channels
General Anaesthesia: Drug Stages
General anaesthesia Different drugs for Premedication; Induction and; Maintenance
Premedication Objectives
Premedication Objectives
- To sedate the patient
- Reduction of anxiety and pain and providing amnesia for post-operative period
- Prevention of parasympathomimetic effects of anaesthesia (bradycardia; salivation; bronchial secretions; coughing; vomiting
- Reduce involuntary muscle contractions
Premedication: Sedatives and Anxiolytics
Premedication Sedative/hypnotic and Anti-anxiety agents Benzodiazepines: Most important group. Provide anxiolysis; sedation; reduction in muscle tone; anterograde amnesia; anticonvulsant effects (e.g. midazolam
GABA Target Receptors
GABA Target GABA-A receptors Barbiturates Neuroactive Steroids + Benzodiazepines Picrotoxine Synaptic cleft Cytoplasm CI- a1-6, B1-4, 1-3, 8, E, 0, 1 and p1-3
Premedication: Analgesia and Antagonists
- Analgesia: Opioids remain the mainstay due to the severity of surgical pain Used pre- and post-operatively Morphine; fentanyl Post-operative S/E include constipation; urinary retention; respiratory depression; nausea and vomiting
- Muscarinic antagonists: Prevent excessive cholinergic effects such as salivation and bronchial secretions. Also protect the heart from arrhythmias caused by some anaesthetics like halothane (e.g. Atropine; hyoscine)
- Antiemetic drugs: Prevent post-operative vomiting (e.g. Metoclopramide; prochlorperazine)
Premedication: Neuromuscular Blockers
- Neuromuscular blockers Prevention of reflex-induced muscle contractions for abdominal/thoracic surgery Tracheal intubation NMBs block synaptic transmission at the neuromuscular junction (nACh receptors. Two classes: Non depolarising: act by blocking nACh receptors directly (antagonists) e.g. Pancuronium; vercuronium; atracurium Depolarising: act as agonists at nACh receptors. Initial effect is depolarisation (muscle fasciculation) then nerve block due to its sustained presence (not broken down by AChE) and activation of the receptor. e.g. succinylcholine
Neuromuscular Junction Diagram
AcCoA Choline Vesamicol CAT CoA ACh ACh carrier e ACH Empty vesicle Choline carrier Exocytosis Presynaptic toxins, e.g. botulinum Hemicholinium ACh leak ACh AChE Choline + Acetate Non-depolarising blocking agents, e.g. tubocurarine + Depolarising blocking agents, e.g. suxamethonium Anticholinesterases e.g. neostigmine Na+ K+ Postsynaptic nicotinic ACh receptor @ Elsevier. Rang et al: Pharmacology 6e - www.studentconsult.com Presynaptic nicotinic ACh receptor
General Anaesthetics: Classes
General Anaesthetics · There are 2 classes: 1. Intravenous Anaesthetics - Injections - Anaesthetics or induction agents 2. Inhalation Anaesthetics - Gasses or Vapors - Usually Halogenated
General Anaesthetic Agents: Intravenous
General Anaesthetic agents Intravenous Used for induction of anaesthesia because: 1. Act rapidly (~ 20-30 seconds) 2. Less traumatic for patients 3. Short duration of action-about 10 minutes for each dose. Not suitable for long-term maintenance of anaesthesia
Intravenous Agents: Propofol and Etomidate
General Anesthetic agents Intravenous · Propofol Most widely used Rapidly distributes to brain, so quick onset of action. Rapidly metabolised so in some cases can be used for induction AND partial maintenance No need for NMB Less postoperative drowsiness, nausea and vomiting Both thiopental and propofol cause respiratory depression of cardiac output · Etomidate Thought to act on GABA-A receptors containing the beta3 subunit Short acting => rapid induction and recovery Used for induction of general anaesthesia or sedation during minor procedures which do not require general anaesthesia Major advantage is less cardiovascular and respiratory depression No analgesia so use opioids May cause adrenorcortical suppression by inhibiting steroidogenesis
General Anaesthetic Agents: Inhalational
- Used for Maintenance of anaesthesia
- Administered in gaseous form . No need for metabolism before elimination by lungs => preferred for maintaining anaesthesia
- Elimination occurs via expired air => rapid decrease of brain and cardiac concentration and reversal of anaesthetic effect
- Administered at a particular gas or vapour pressure rather than a dose
- At steady state, gas concentration in lung correlates with brain concentration => monitor end-expiratory gas concentration to monitor brain concentration. Not possible with intravenous anaesthetics
Inhalational Agents: Nitrous Oxide and Isoflurane
- Nitrous oxide (laughing gas N20) Many advantageous features for anaesthesia widespread use Rapid in action Is analgesic in sub-anaesthetic doses. 50% mixture with oxygen is used when analgesia is required (e.g. Childbirth) Not potent enough to be used alone so often combined with lower concentrations of other agents Has little effects on cardiac and respiratory system => low S/E profile
- Isoflurane Widely used Produces anaesthesia, analgesia as well as muscle relaxation ➢ Binds to GABA, Glutamate receptors. Also affects potassium channels. Causes hypotension due to vasodilatation though less than Halothane Does not sensitize the heart to adrenaline like halothane Muscle relaxation Can irritate mucous membranes Preferred inhalational anaesthetic in obstetrics
Inhalational Agents: Desflurane and Sevoflurane
Desflurane Chemically similar to isoflurane Lower potency than isoflurane Recovery from anaesthesia is rapid due to its low solubility Not recommended for induction due to its irritant nature to upper respiratory tract
- Sevoflurane More potent and less respiratory tract irritation than desflurane Sevoflurane Rapid acting and more potent than Desflurane Rapid recovery from anaesthesia Non-irritant so can be used for induction Has little effect on heart
Regional and Local Anaesthesia
Regional/Local Anaesthesia
Local Anaesthesia Objectives
Local Anaesthesia OBJECTIVES · interruption of pain impulses in a specific region of the body without a loss of patient consciousness. · Completely reversible -- the agent does not produce any residual effect on the nerve fiber
Synaptic Block in Local Anaesthesia
Synaptic block: · + presynaptic Ca2+ entry -¿ transmitter release · + postsynaptic CI- entry and + K+ outward leakage -> inhibition general anesthetic
Conduction Block in Local Anaesthesia
Conduction block: local anesthetic · + axonal Na+ entry -> failure of action potential propagation
Mechanism of Action of Local Anaesthetics
Mechanism of Action Local anaesthetics block nerve conduction
Action Potential in a Neuron
Chapter 13 Opener Principles of Anatomy and Physiology, 11/e 2006 John Wiley & Sons Na channel open Na channel closed 1 Dendrites Cell Body Axon Hillock Myelin Sheath Membrane Potential (mV) - depolarization repolarization 0 threshold potential -50 resting potential resting potential hyperpolarization -100 0 1 2 3 4 5 6 7 Time (milliseconds) Action Potential in a Neuron action refractory potential period 50
Local Anaesthetics Blocking Na Channels
Mechanism of Action Local anaesthetics block nerve conduction by blocking Na channels Exterior Axonal Menbrane Interior B B B Na+ H+ BH+ BH+ Channel open Hydrophobic pathway (no use-dependence) Hydrophilic pathway (use-dependent) Na+ BH+ BH+ Channel shut H+ B B B B=blocking agent @ Elsevier. Rang et al: Pharmacology 6e - www.studentconsult.com
Sodium Ion Influx Inhibition
Mechanism of Action . Local anaesthetics block nerve conduction by reducing the influx of sodium ions into the nerve cytoplasm. · Sodium ions cannot flow into the neuron, thus the potassium ions cannot flow out, thereby inhibiting the depolarization of the nerve. . If this process can be inhibited for just a few Nodes of Ranvier along the way, then nerve impulses generated downstream from the blocked nodes cannot propagate to the ganglion.
Types of Local Anaesthesia
Local Infiltration and Surface Anaesthesia
Types of Local Anaesthesia Local Infiltration (Local Anaesthesia). . Nerve endings in the skin and subcutaneous tissues are blocked by direct contact with a local anaesthetic · Used primarily for surgical procedures involving a small area of tissue (for example, suturing a cut). · Lidocaine;benzocaine; tetracaine Surface Anaesthesia · Application of a local anesthetic to skin or mucous membranes. · Surface anesthesia is used to relieve itching, burning, and surface pain (for example, as seen in minor sunburns). · Lidocaine; benzocaine; tetracaine
Topical Block and Nerve Block
Types of Local Anaesthesia Topical Block · Anaesthetic agent applied directly to mucous membrane surface (cornea; respiratory tract; oral mucosa) · Used during examination procedures (often in spray form) . Lidocaine; tetracaine; benzocaine Nerve Block . Local anaesthetic is injected around a nerve that leads to the operative site. . More concentrated forms of local anaesthetic solutions are used for this type of anesthesia. . Used for surgery or dentistry · Lidocaine;bupivacaine
Epidural and Spinal Anaesthesia
Types of Local Anaesthesia Epidural Anaesthesia · Accomplished by injecting a local anaesthetic into the epidural space. · The epidural space is above the dura and surrounds the spinal cord. · Lidocaine; bupivacaine SPINAL CORD: Gray matter White matter Posterior median sulcus Spinal Central canal Anterior median fissure Spinal nerve SPINAL MENINGES: Pia mater (inner) Denticulate ligament Arachnoid mater (middle) Subarachnoid space Dura mater (outer) Subdural space Anterior view and transverse section through spinal cord Figure 13-1a Principles of Anatomy and Physiology, 11/e @ 2006 John Wiley & Sons Anaesthesia Local anesthetic is injected into the subarachnoid space of the spinal cord to act on spinal roots and spinal nerves . Acts more quickly than epidural anaesthesia . Used for surgery to abdomen, pelvis or leg if GA is contra-indicated • Mainly lidocaine
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
