Diabetes: Pathophysiology, Glucose Metabolism, and Insulin Production
Document from University about Diabetes. The Pdf explores the pathophysiology of diabetes, covering glucose metabolism, insulin production, and the disease's history. This Pdf, suitable for University students studying Biology, includes tables and diagrams to clarify biological processes and differentiate between type 1 and type 2 diabetes.
Mostra di più16 pagine


Visualizza gratis il Pdf completo
Registrati per accedere all’intero documento e trasformarlo con l’AI.
Anteprima
Diabetes Mellitus
The lecture is based on the latest evidence-based findings found in this edition of Diabetes Care.
Glucose Metabolism: Pathophysiology
It is relevant for energy purposes. ATP provides energy; it derives from glucose metabolism; glucose is present in the blood.
Krebs cycle and oxidative phosphorylation are the main producers of ATP molecules.
Blood glucose derives from 3 sources:
- food glucose: starch and disaccharides are found in food; they are absorbed and flow in the blood.
- glycogen: to maintain homeostasis
even when we don't eat; found in
- muscle: to provide energy to the muscle;
- liver: to maintain normal glucose levels): to maintain homeostasis;
- from gluconeogenesis: using different substrates (mainly proteins but also lipids) to produce glucose; performed in the liver only
Hormone Metabolic Effects on Glycemia
HORMONE ORIGIN METABOLIC EFFECT GLYCEMIA INSULIN pancreas B cells 1 glucose entrance in cells; 1 glycogensynthesis, liposynthesis, proteosynthesis; 4 glycogenolysis gluconeogenesis, proteolysis, lypolysis GLUCAGON pancreas a cells 1 glycogenolysis; 1 gluconeogenesis 1 SOMATOSTATIN pancreas 6 cells inhibits release of glucagon, insulin, pituitary trophic hormons, gastrin, secretin 1 EPINEPHRINE adrenal medulla î glycogenolysis; 1 lypolysis 1 CORTISOL adreno- cortical 1 gluconeogenesis; insulin antagonist 1 ACTH anterior pituitary anterior pituitary 1 cortisol; 1 lypolysis 1 GH insulin antagonist THYROXINE thyroid 1 glycogenolysis; 1 carbohydrates absorption 1
Glycemia Regulation
GLYCEMIA - is kept within a narrow range thanks to specific hormones . anabolic-> insulin: is the only hormone decreasing glycemia by causing cells to absorb glucose (without insulin cells would be impermeable to glucose) . hyperglycemic hormones; metabolic/catabolic; boost cell activity and are divided in 3 groups:
- glucagon and somatostatin: increase glycemia by increasing glycogenolysis and gluconeogenesis; and by decreasing insulin secretion)
- Glucagon, somatostatin, and insulin (anabolic) are all released by pancreatic cells.
- stress hormones-> noradrenalin, cortisone and ACTH: involved in fight or flight reaction base
- GH and thyroxin: secreted by pituitary gland and thyroid gland; either direct antagonist of insulin release or increase glycogenolysis and carbohydrates absorption.
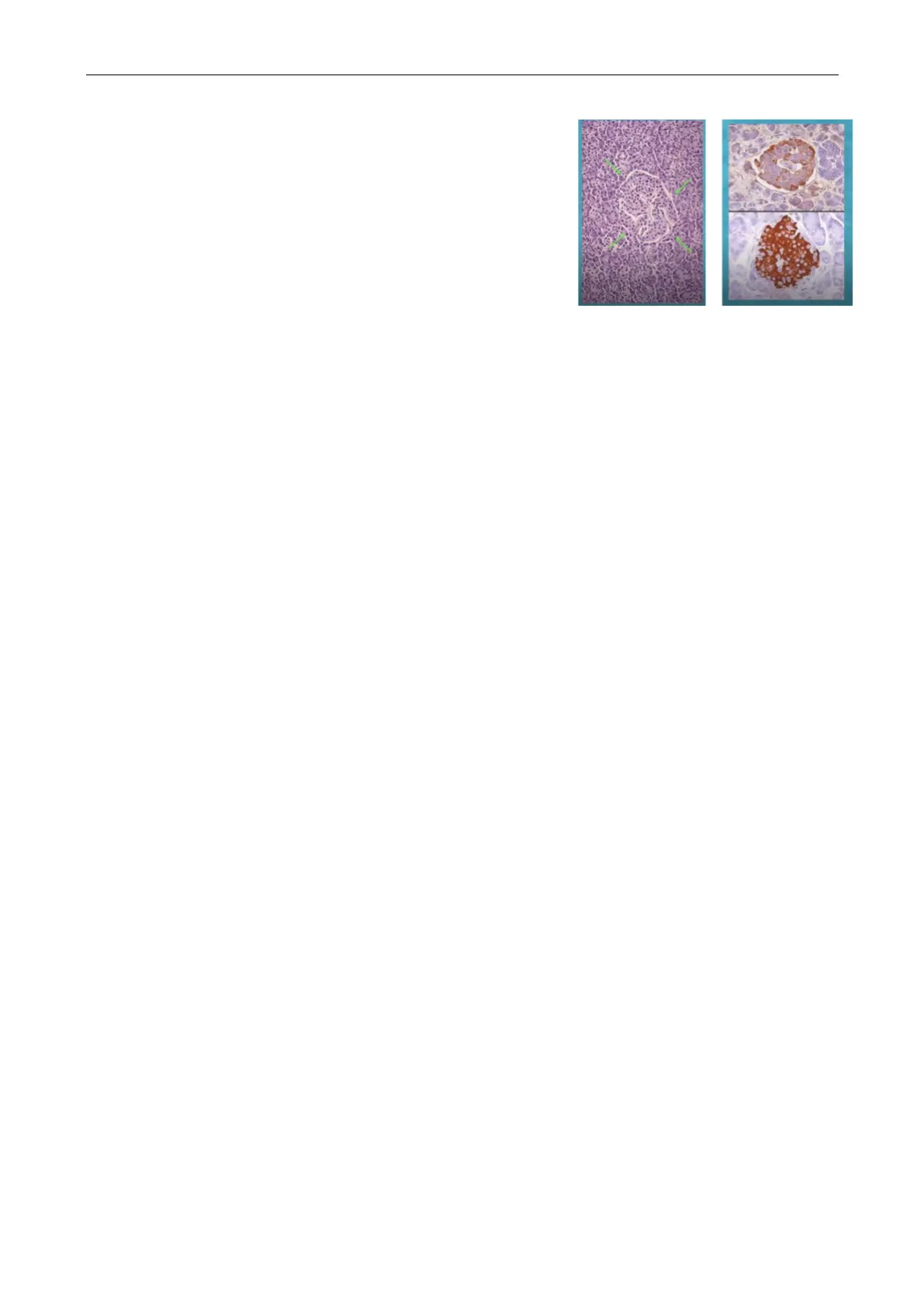
Histology of Pancreatic Islands
In the picture hematoxylin and eosin staining; pancreas has 2 components
Exocrine Pancreas
- displays adenomers: glandular cells featured by nucleus located in the base of the cell (above);
Endocrine Pancreas
- cells display a central nucleus (below)
Exocrine and pancreas are separated by a thin basement membrane (cannot be seen in light microscope) and lined by vessels
There are 2 ways to distinguish the cells of Langerhans islets:
- histochemistry: Mallory trichrome
- immune histochemistry: employs monoclonal antibodies binding the
those cells are:
- beta cells: 80% insulin positive
- alpha (glucagon) or delta (somatostatin): 10-15%: scattered in the periphery
History of Diabetes
Diabetes is a condition which has been known for 3000 yrs.
- Egyptians: Ebers papyrus provides the 1st description of diabetes-> symptom of this disease included frequent urination
- Indians: Indu claimed that urine attracted ants. Diabetes was considered as an emaciating disease: this is because people with diabetes (especially T1DM) would lose fluid and perform gluconeogenesis to produce glucose needed by cells. Hence, cells would end up being destroyed because they had no access to glucose.
- V century BC: 1st description of T2DM (obesity related). They tasted urines-> urines were sweet in taste-> they derived the connection bw diabetes and glucose. [water testers did their (sweet and rewarding) job up to the 11th century]
- 250 BC: Apollonius of Memphis coined the term Diabetes; the word derives from the Greek verb "diabaino" standing for "going through". This is because diabetic people drink a lot of water hence urinate a lot (water passes through ;)).
- Il century BC (Christian era): Areteus described diabetes as a melting down of flesh and limbs into urines (as Indians already said)
- 164 AD: Galen performs the 1st diabetes diagnosis. erroneously believing that diabetes was due to kidney
- 11th century: the adjective melllitus (latin) was added to the noun diabetes (Greek) meaning as sweet as honey [just the way you are, nfs]
- 16th century: Paracelsus was 1st to understand that diabetes is not associated with kidney
- 1667: Dobson (oxford school): by performing the evaporation of diabetic urines > they found sweet crystals present in both urines and blood [at the time you had both water tasters and blood testers, sort of vampires]. At this point, diabetes was classified into:
Diabetes Classification by Dobson
- Fatal (in 5-8 weeks)> acute-> type 1 DM
- Non-fatal-> Chronic-> type 2 DM
- Early VII century: Rollo (a Switzerland physician) who provided the 1st dietary treatment to diabetes
- 1869: Langerhans understood that pancreas was made by an exocrine component (secreting fluids) and another component (however, didn't understand the function of this second one)
- 1989: Minowski and Von Mering performed removal of dog's pancreas and discovered that, in this way, food digestion was impaired, and diabetes developed
- 1908: Zuelzer extracted a "substance" (insulin) from pancreas; it was injected to into 5 diabetic patients. Those patients remitted, however crude extraction with enzymes caused people to develop side effects.
- 1909: the "substance" was given the name of insulin by de Mayer of Belgium
- 1921: 1st isolation of insulin in Toronto university (where they developed a successful process of inactivation of polio virus) performed by Banting and Macleod-> It was the beginning of diabetic therapy with insulin
Classification of Diabetes Mellitus
Formulated by the American diabetic association, in 1910 and publish in Diabetes Care in 1943. [Professor will make references to the updates that came up in the last 30 yrs > the newest ones being dated back to 3 months ago]
- type 1: autoimmune destruction of beta cells-> absolute insulin deficiency. Includes LADA aka latent diabetes of adulthood.
- type 2: progressive decrease of beta cells insulin secretion; the background is insulin resistance. Usually associated with metabolic syndrome
- specific types (more than 100): 2% of overall
patients; involve:
- genetic defects: beta cell function or insulin faction
- diseases of exocrine pancreatitis: e.g. acute and chronic pancreatitis
- endocrinopathies
- drug or chemical (glucocorticoids, diazine diuretics or HIV therapy) induced: increasing in numbers;
Other Specific Diabetes Types
Ill. Other specific types E. Drug or chemical induced A. Genetic defects of B-cell function 1. Vacor 1. Chromosome 12, HNF-la (MODY3) 2. Pentamidine 2. Chromosome 7, glucokinase (MODY2) 3. Nicotinic acid 3. Chromosome 20, HNF-4a (MODY1) 4. Glucocorticoids 4. Chromosome 13, Insulin promoter factor-1 (IPF-1; MODY4) 5. Thyroid hormone 5. Chromosome 17, HNF-18 (MODYS) 6. Diazoxide 6. Chromosome 2, NeuroDI (MODY6) 7. B-adrenergic agonists 7. Mitochondrial DNA 8. Thiazides 8. Others 9. Dilantin B. Genetic defects in insulin action 10. y-Interferon 1. Type A insulin resistance 2. Leprechaunism 3. Rabson-Mendenhall syndrome 4. Lipoatrophic diabetes 5. Others C. Diseases of the exocrine pancreas 1. Pancreatitis 1. "Suff-man" syndrome 3. Neoplasta 4. Cystic fibrosis 5. Hemochromatosts 6. Fibrocalculous pancreatopathy 7. Others D. Endocrinopathies 1. Acromegaly 4. Wolfram syndrome 2. Cushing's syndrome 5. Friedreich ataxia 3. Glucagonoma 6. Huntington chorea 4. Pheochromocytoma 7. Laurence-Moon-Bledl syndrome 5. Hyperthyroidism B. Myotonic dystrophy 6. Somatostatinoma 9. Porphyria 7. Aldosteronoma 8. Others 10. Prader-Willi syndrome 11. Others
- infection
- other uncommon immune mediated forms
- other genetic syndromes: e.g. Down and Klinefelter syndromes
- gestational: diagnosed in the 2nd or 3rd trimester of pregnancy in previously non-diabetic women
Uncommon Forms of Diabetes
G. Uncommon forms of immune-mediated diabetes 2. Trauma/pancreatectomy 2. Anti-Insulin receptor antibodies 3. Others H. Other genetic syndromes sometimes associated with diabetes 1. Down syndrome 2. Klinefelter syndrome 3. Turner syndrome 11. Others F. Infections 1. Congenital rubella 2. Cytomegalovirus 3. Others
Differences Among Type 1 and Type 2 Diabetes
Mind that old-fashioned definitions such as juvenile and elderly diabetes are no longer used
T1D T2D causes ฿ cell destruction insulin resistance circulating insulin reduced to absent increased/normal/reduced onset acute progressive age mostly young prev. > 40 inheritance limited high obesity absent present onset symptoms present, prominent absent or light acute complications ketoacidosis hyperosmolar hyperglycemic nonketotic syndrome chronic complications years after onset frequently at diagnosis prevalence absolute 0.3-0.6 % 3-7 % relative <10 % >90 % gender M=F M<F therapy insulin diet+exercise, oral drugs, insulin
Type 1 Diabetes Characteristics
- No gender association (same incidence in males and females)
- Limited inheritance
- No association with obesity
- Complication: ketoacidosis
> Since complications take year to manifest, diagnosis is generally performed later in life
Type 2 Diabetes Characteristics
2:
- Aetiology: insulin resistance leading to
- (at the beginning): increased insulin production-> when the pancreas can no longer bear this condition insulin levels go back to normal, but then decrease leading to the onset of clinical diabetes (the onset is progressive)
- >40 yrs old: no longer completely true; on account of risk factors now affecting the general populationalso young people (in their 20s or 30s) can be affected by T2DM
- More common in females
- MAIN DIFFERENCE WITH RESPECT TO T1DM: There's still little production of insulin-> hence, little entrance of glucose in the cell-> no ketoacidosis
- Complication: hyperosmolar hyperglycemic non ketonic syndrome
- Diagnosis comes after complications
Insulin Production Process
- Produced
- as pre-pro-insulin: 110 aas polypeptide; 11.5 kdalton molecular weight
- in endoplasmic reticulum-> then it moves to Golgi-> there it is processed
- cleavage of signal peptide-> 2) formation of disulfide bonds->
- production of pro-insulin: (86 aas; 9 kda)-> 4) New cleavage in golgi: producing c-peptide aka chain c peptide and mature insulin.
In the vesicles deriving from Golgi apparatus you can find an equimolar concentration of insulin and c peptide.
Mature Insulin
MATURE INSULIN Pro-Insulin Human Insulin 7 - 1: · Aetiology: beta-cell destruction · Acute . Affects mostly young people.
Non hai trovato quello che cercavi?
Esplora altri argomenti nella Algor library o crea direttamente i tuoi materiali con l’AI.
