Broncopneumopatia Cronica Ostruttiva: definizione, epidemiologia e patogenesi
Documento sulla Broncopneumopatia Cronica Ostruttiva (BPCO). Il Pdf esplora la definizione, l'epidemiologia, le cause di mortalità e la patogenesi della BPCO, inclusa l'infiammazione e il rimodellamento delle vie aeree. Vengono anche discusse le differenze tra BPCO e asma a livello patologico, utile per lo studio universitario.
Mostra di più15 pagine

Visualizza gratis il Pdf completo
Registrati per accedere all’intero documento e trasformarlo con l’AI.
Anteprima
COPD: Definizione e Caratteristiche
COPD is an acronym that means "Chronic Obstructive Pulmonary Disease" and it is like an umbrella because under this we have many diseases and the main ones are Chronic Bronchitis and Emphysema but among them, we have a lot of mixed Pathological presentations of Obstructive Diseases.
Definizione di BPCO
COPD is a common preventable and treatable disease and it is characterized by Persistent Airflow Limitation so we are talking about Spirometry and this Airflow Persistent Limitation is usually progressive and it means that it goes further over the years and is associated with an enhanced Chronic Inflammatory Response_it means that this is an Inflammatory Disease and the Inflammation is the main part of the disease itself. This Inflammation is mainly located in the Airways but we can see it also in the Parenchyma and the Lung to noxious particles or gases so it happens because of something that we have inhaled and goes in the Airway or deep in the Lung, in the Parenchyma. Then there are some particularly events in COPD that are called Exacerbations so acute phases of the Disease and they affect very much the natural course of the disease. We have also Comorbidities because in COPD we are dealing with a mature group of Patients, they are aged and they are affected by multiple conditions so Comorbidities affect a lot the Disease itself but also the course of the disease. So, Comorbidities and Exacerbations contribute to the overall severity in individual patients. We have to look at COPD as a very complex condition and we have to evaluate the individual affected by COPD in a sort of holistic way so we cannot see or look at the Obstructive Disease without looking at all the other things the patient is affected with.
Impatto della BPCO
COPD although is one of the most common diagnoses that you can find in a Patient that has a certain age and not always is appropriate, it is a leading cause of Morbidity and Mortality worldwide. The burden of COPD is projected to increase in the coming decades due to continued exposure to COPD risk factors and the aging of the world's population. We are dealing with the aging of the population because Science is improving in this knowledge very much. COPD is also associated with a significant Economic Burden because they are using very much resources so Hospitals, Clinics, Rehabilitation, Pharmaceutical expenses that affect very much the community especially in a country like Italy where we have a Public Health System so we are paying with Taxes all of this. It is affecting the Economical point of view in a completely different way compared to Asthma because in Asthma we are evaluating in one of the aspects related to the Economic part how many days of work this Individual was losing or days of school lost. In this case, since we are dealing with a population of mainly old Individuals, they are affected not because of their active life in terms of work but because they are using many Health resources.
Cause di Morte e BPCO
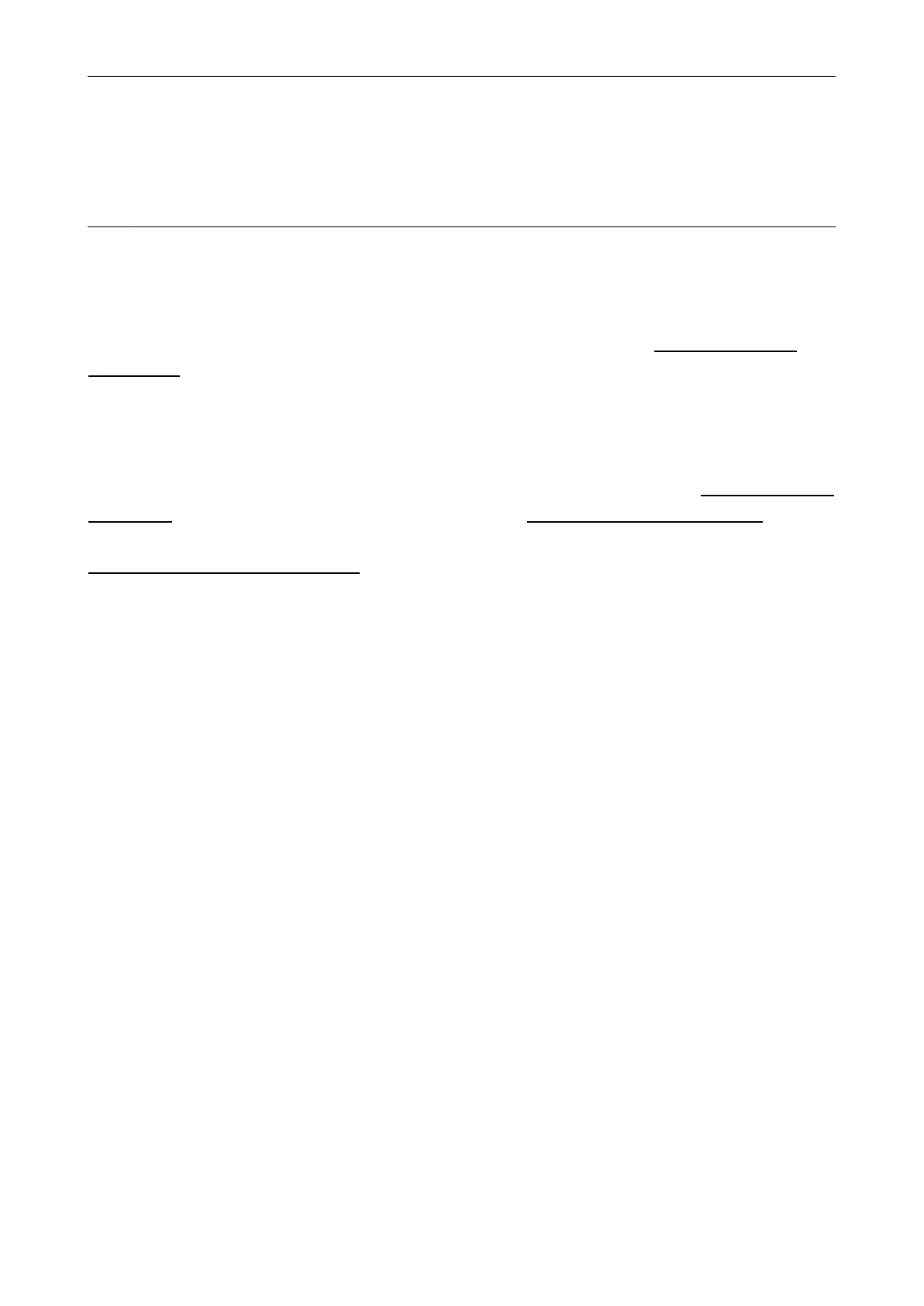
Le 10 cause di morte più comuni
This graph takes into consideration the West European countries. Vascular conditions like Ischemic Heart Disease and Cerebrovascular Disease are the main ones but beyond that, we have Respiratory conditions that are Lower Respiratory Infections and also COPD that are affecting very much Individuals for the major outcome that is survival.
Deaths attributed to Worldwide WHO European Region Ischaemic heart disease 7.3 million (12.8%) 2.40 million (24.7%) Cerebrovascular disease 6.2 million (10.8%) 1.40 million (14.0%) Lower respiratory infections 3.5 million [6.1%) 0.23 million (2.3%) COPD 3.3 million (5.8%) 0.25 million (2.5%) Diarrhoeal diseases 2.5 million (4.3%) 0.03 million (0.3%) HIV/AIDS 1.8 million [3.1%) 0.08 million (0.8%) Trachea/bronchus/lung cancer 1.4 million (2.4%) 0.38 million (3.9%) Tuberculosis 1.3 million (2.4%) 0.08 million [0.8%) Diabetes mellitus 1.3 million (2.2%) 0.17 million (1.7%) Road traffic accidents 1.2 million (2.1%) 0.12 million [1.2%) Other Pulmonary vascular disease 0.8% respiratory 0.19 ILD 0.4% Pneumoconioses 0.3% Acute LRI Cardiovascular disease 40% Pneumonia 3.5% Flu Asthma 0.2% Respiratory deaths 15% Other deaths 24% Nonrespiratory cancers 21% Lung cancers 5.8%
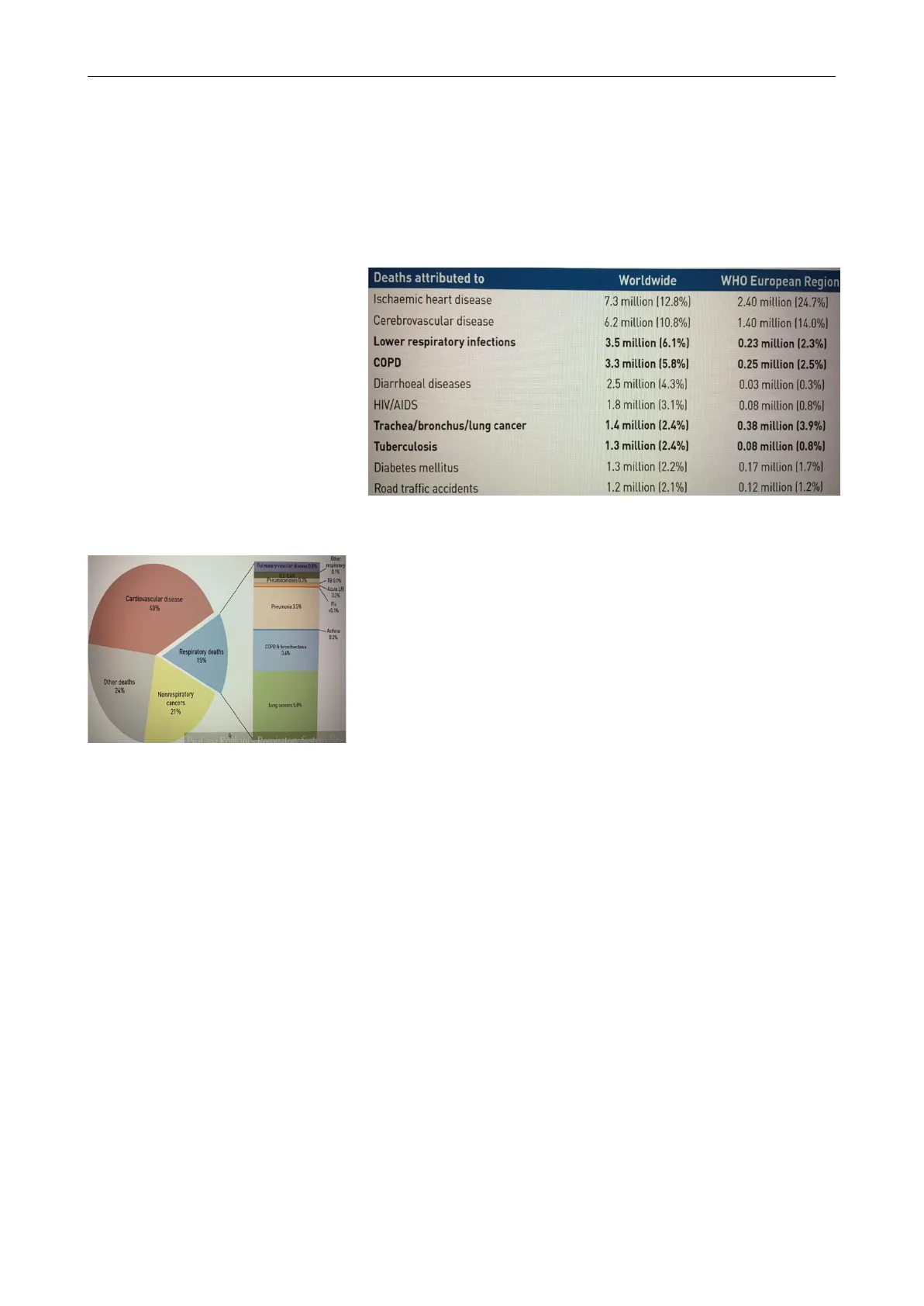
Percentuale di decessi per condizione respiratoria in Europa
Here we have COPD and Bronchiectasis where the mortality is 3,4% so just beyond Pneumonia (3,5 %) and Lung Cancer (5,8%).
Storia Naturale della BPCO
COPD has a variable natural history and not all individuals follow the same course because there are different conditions under this umbrella. But the thing is that all of them are progressive and it is increasingly that COPD often has its roots decades before the onset of symptoms, it means that it is something very slow that happens over years before it becomes clinical evident and this happens actually in a sort of Young-Adult age. The Young smokers between the 3rd and the 4th decades so between the 30 and 40 years the damage will become evident later on, it became to take place there in a Smoker because Smoking Habits is one of the main major risk factors in COPD and this is why it's preventable because we can take away most of those risk factors so we can prevent this Disease. Impaired growth of Lung function during childhood and adolescence caused by recurrent infections or Tobacco smoking, may lead to lower maximally attained Lung function in early Adulthood and this is another risk factor that is evolving very much and is taking a lot of attention for impairing Lung function because it appears that the possibility that a specific individual will be affected by COPD start even earlier than Young Adult. In a new theory, it seems that we have to pay attention to what is called the "Epidemy of Preterm Birth" that will have a sort of impaired Lung Function since the beginning because it happens to people that are born with Small Lungs and these Small Organs will be less efficient compared to a full developed organ and although this Individual, in a recent Epidemiological study, it has been highlighted that they will have a small Lung function compared to a Normal Individual during the entire life. But if this specific individual starts to be affected by specific risk factors that can be self-inflicted like Cigarette smoke, then the problem will be clinically evident decades before the Normal Individual. So the Doctor should be very careful when interrogating a Patient in asking everything since it's born like for example "Are you a Preterm Baby?" should be one of the first questions to ask. So this abnormal growth will, often combined with a shortened plateau phase in teenager smokers, increase the risk of COPD.
Importante studio sulla storia naturale
This is a very important paper that was published a few years ago that pointed out the specific aspect that everything will happen in normal or not normal growth of the Lung will affect later on the slope of Lung function over time. The age doesn't start with 0 so when the child is born but even earlier so when the Baby is in the Womb and the Green Line is the one that represents the development of the Lung and then in terms of Normal or Abnormal Lung development there is an aging of the Lung that is physiologically declined. We have also the Red Line that intercepts the normal slope of the Lung function over time that can affect this very much and is due to many things, especially the Environment and it seems that there is a sort of interaction between this and Specific Gene interactions. Although we do not have a specific Gene that is the gene of the disease of COPD, we have different Genes and some of them are very much related and only 1 Gene we know for sure that is able to induce a Disease that is among COPD Emphysema and that Gene is a1-antitrypsin so the deficiency in it is able to induce Genetic Related Disease Emphysema but it is a very rare condition and we have to found the Individual affected by this specific deficiency in a Homozygous status because the Heterozygous not always will lead to the Disease. So in this Paper, it is very interesting because it highlights the Individual that is Environment (E)TS & genes usually born Preterm or a baby Environment (E)TS & genes that has an impaired Lung development that is near to normal and they happen to Environment ETS & genes have Lung function slower than Environment (E)TS & genes a Normal Individual and this -1 0 1 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 Age doesn't mean that this Individual is sick but it is much Genes leading to abnormal lung development & lung growth more prone to develop COPD even earlier than a normal Genes for: Genes for: Inflammation Airway remodeling Asthma -COPD Mucous production Small airway disease Emphysema (Allergic) inflammation. Airway remodeling Small airway disease individual and if this specific Individual with this impair or reduced Lung development will be intercepted with a specific risk factor, then it will be very sick.
This is a paper that has been --- Never smoked or 75 Smoked regularly and susceptible to the effects not susceptible to smoke published in 1977 and was pointed out that Risk Factors are affecting very much Lung 50 - Onset of symptoms function in a progressive way Stopped smoking at age 45 years that is irreversible in the 25 Severe disability Stopped smoking at age 65 years damage that affects the Airway or the Parenchyma and we can Death 0 50 25 75 FEV1 (% of value at age 25 years) Age (years) detect that using a very simple and non-invasive test that is "Spirometry" that can give us a lot of information regarding what is happening in Lungs and Respiratory Functions of our Patients. We can see the age of the Patients from 25 to 75 and we have the FEV1 so the main parameter that we use to monitor the severity of Obstructive Conditions. The Line in the Bluish area is a normal slope of Lung function in a normal individual who never smokes so the decline is only given by the aging process so it is a normal process. The Black Line instead represents a Young Smoker that usually smokes a pack a day, so 20 cigarettes per day. In the first year, he doesn't even feel a problem because usually till 50 years old it reaches like 75-70% of what is supposed to have in terms of FAV1 but if we continue to smoke then we will have the onset of Symptoms so the Individual, at the age of 60, will refer to his Doctor because he starts to have cough and sputum in it due to Inflammation and maybe he also start to have Dyspnea on exertion, it means that if we go to the 3rd floor using the stairs he must stop and rest before reaching the floor. If the Individual continue to smoke, then when the FEV1 is below 30%, severe disability happens so he will start experiencing Dyspnea when he just walks on a flat surface. If the Individual stop to smoke the slope of the curve will never go back to a normal rate. It would reduce the decline that is not as fast anymore as before. So it is never too late to stop smoking for our Patient but if he would never smoke it would have been much better. This is the first paper that pointed out this very important aspect of how risk factors can irreversibly affect the Lung function of our individual in terms of Obstruction and the feature of Obstruction in COPD is that it is Irreversible compared to Asthma that instead is Reversible. An accelerated decline in Lung function is nevertheless still the single most important feature of COPD that generally is a progressive disease, especially in the patient exposure to noxious substances, most often Tobacco, continues. If exposure is stopped, the disease may still progress mainly due to the decline in Lung function that normally occurs with aging. Nevertheless, stopping exposure to noxious agents, even after significant airflow limitation is present, can result in some improvement in function and will slow or even hold the progression of the disease.
Fattori di Rischio per la BPCO
Non hai trovato quello che cercavi?
Esplora altri argomenti nella Algor library o crea direttamente i tuoi materiali con l’AI.
