Multiple Sclerosis: Pathology, Therapeutic Strategies, and Pharmacological Treatments
Slides from University about Multiple Sclerosis. The Pdf provides a detailed overview of multiple sclerosis, including its pathology, therapeutic strategies, and pharmacological treatments. This University-level Biology document, produced with clear digital text and sharp images, is useful for self-study.
See more31 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
MULTIPLE SCLEROSIS
MULTIPLE SCLEROSIS
- Chronic inflammatory demyelinating pathology of the Central Nervous System (CNS) first described by Charcot in 1868
- Called "Multiple Sclerosis", due to the presence of sclerotic plaques (lesions) disseminated in the white matter of the brain and spinal cord
- Characterized by wide variability of symptoms
- Likely immune-mediated pathogenesis
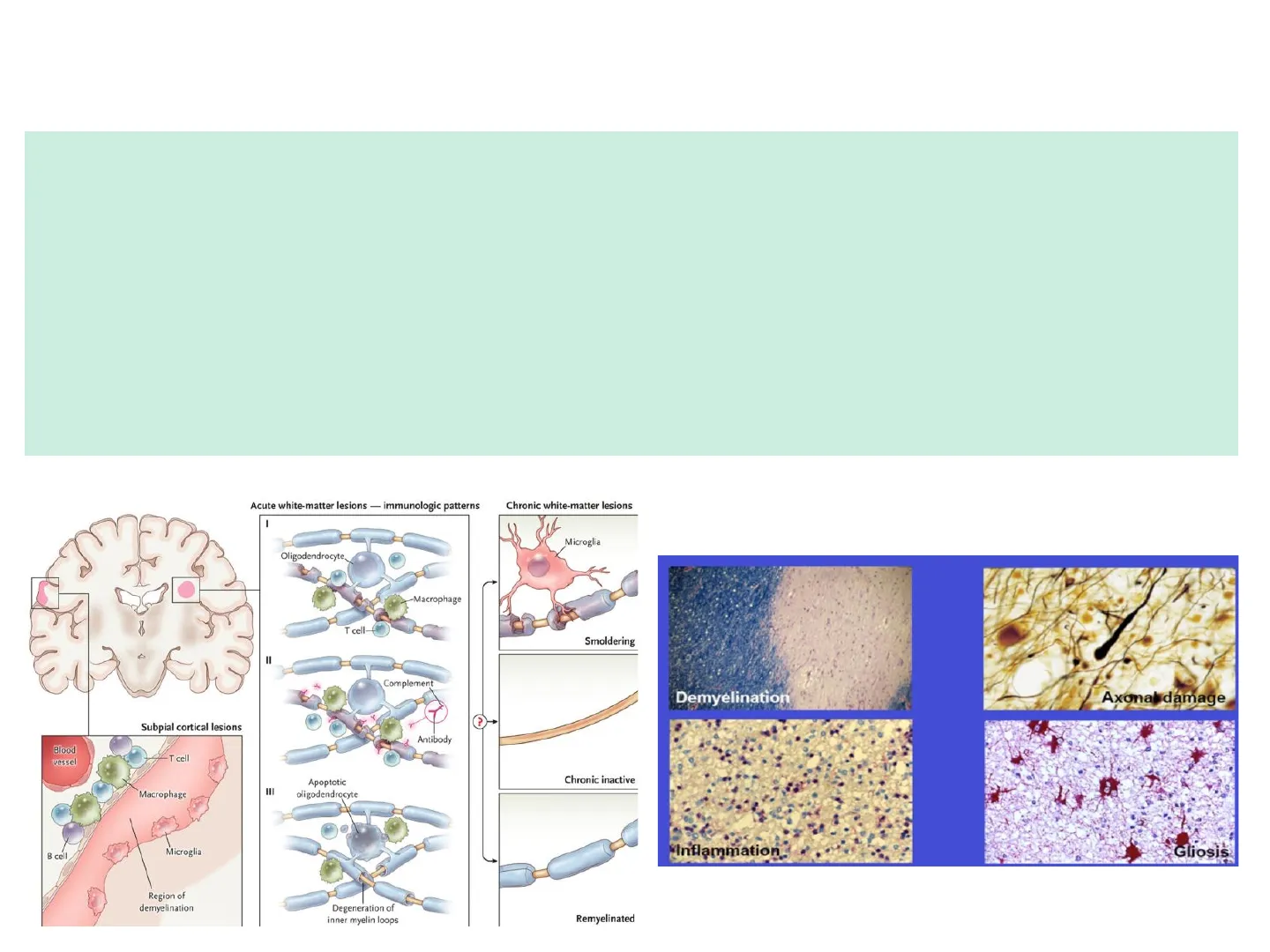
Acute White-Matter Lesions
Acute white-matter lesions - immunologic patterns Oligodendrocyte Macrophage T cell = Antibody Blood vessel -T cell Macrophage B cell Microglia Region of demyelination
Chronic White-Matter Lesions
Chronic white-matter lesions Microglia Smoldering Demyelination Axonal damage Inflammation Gliosis Degeneration of inner myelin loops Remyelinated Reich N Engl J Med 2018 Complement Subpial cortical lesions Apoptotic oligodendrocyte Chronic inactive
Epidemiology of MS
Epidemiology of MS
- Number of people with MS. Prevalence per 100,000 people Unknown 0-25 26-50 51 - 100 101- 200 >200
- There are 2.8 million people living with MS worldwide. 1/8 patients are familiar Concordance in female monozygotic twins is 30% in the UK and Canada, ~8.5% in southern Europe
- in dizygotic twins and siblings 6% and 3% respectively
- RRMS typically onset 20-35 yy
- PPMS typically begins at ~40
- 3-10% in childhood or adolescence http://www.atlasofms.org
- A prevalence of 50-300 per 100 000 people, about 2,3 million people are estimated to live with multiple sclerosis
- Sex ratio has steadily been increasing and it is now close to 3:1 (F:M) in most developed countries
- Migration from low-risk to high-risk regions in childhood is associated with a low risk of developing multiple sclerosis and vice versa
- Minorities in the US, such as Hispanic Americans and black Americans, experience faster disease progression Filippi Nature Rev Primers 2018 Thompson Lancet 2018
Prevalence and Life Expectancy
Epidemiology of MS
- Prevalence estimates range from 2 per 100,000 individuals in Asia to ~1 per 1,000 individuals in Western countries
- A prevalence of 1 per 400 individuals has been reported in some countries with a high latitude
- MS symptoms are the main direct cause of death in >50% of patients with MS, although infections and suicide are substantially increased compared with the general population
- The life expectancy of patients is reduced by 7-14 years, but this decreased life expectancy is less evident in recent estimates
- Most patients presenting in later life (over the age of 60 years) are progressive from onset.
- The prevalence of MS has increased since the 1950s, especially in women, sex ratio has steadily been increasing and it is now close to 3:1 (F:M) in most developed countries
- Comorbidities are frequent in multiple sclerosis and have an adverse influence Dobson EJN 2018 Filippi Nature Rev Primers 2018
Lifestyle and Environmental Risk Factors for MS
Lifestyle and environmental risk factors for MS Risk factor Odds ratio HLA gene interaction Combined odds ratioª Effect during adolescence Immune system implied Level of evidence Smoking ~1.6 Yes 14 No Yes +++ EBV infection (seropositivity) ~3.6 Yes ~15 Yes Yes +++ Vitamin D level <50mM ~1.4 No NA Probable Yes +++ Adolescent obesityb ~2.0 Yes ~15 Yes Yes +++ CMV infection (seropositivity) 0.7 No NA Unknown Yes ++ Night work ~1.7 No NA Yes Yes ++ Low sun exposure ~2.0 No NA Probable Yes ++ Infectious mononucleosis ~2.0 Yes 7 Yes Yes ++ Passive smoking ~1.3 Yes 6 No Yes + Organic solvent exposure ~1.5 Unknown Unknown Unknown Unknown + Oral tobacco or nicotine consumption 0.5 No NA Unknown Yes + Alcohol ~0.6 No NA Unknown Yes + Coffee ~0.7 No NA Unknown Yes + Migration studies consistently support MS being secondary to an environmental exposure Filippi Nature Rev Primers 2018
MS Genetics
MS genetics
- The main genetic is HLA-DRB1*15 and/or other loci in strong linkage disequilibrium with this allele. Heterozygotes for HLA-DRB1*15:01 have an odds ratio of MS >3 and homozygotes >6, yet the mechanism remains unknown (via antigen presentation)
- Protective effects of class 1 alleles (e.g. HLA-A*02:01)
- Genome-wide association studies have identified more than 200 single nucleotide polymorphisms associated with MS susceptibility
- The HLA locus accounts for 20-30% of the genetic susceptibility in MS
- IL2R and IL7R, CD58, TYK2, STAT3, and TNFRSF1A (tumor necrosis factor receptor super family 1A (TNFRSF1A)) (non-HLA associations)
- Polymorphisms in genes involved in T cell activation and proliferation (such as IL2 and IL7R) are a major feature of the disease
- Polymorphisms in genes involved in vitamin D metabolism (such as GC and CYP24A1)
- Mutations in only a few genes that have clear functions in the nervous system have been associated with an increased risk of MS (MANBA and GALC) Baranzini Trends in Genetics 2017
Autoimmunity Gene Network
Autoimmunity Gene Network Autoimmune lymphoproliferative syndrome Type 1 diabetes Primary biliary cirrhosis Multiple sclerosis Autoimmune hepatitis Behcet disease Myasthenia gravis Celiac disease Crohn disease Systemic lupus erythematosus Inflammatory bowel disease Rheumatoid arthritis Ankylosing spondylitis Ulcerative colitis Graves disease Psoriasis Autoimmune thyroiditis Thrombocytopenia purpura All known associations with common autoimmune diseases were obtained from the Genome-Wide Association Study (GWAS) and mapped to the closest or most likely affected gene Baranzini Trends in Genetics 2017
Pathophysiology of MS
Pathophysiology of MS
- Inflammation in MS only affects the CNS
- Genetic and pathological studies point towards the adaptive immune system (T cells and B cells)
- The innate immune system, mainly consisting of phagocytic cells, also has an important role in the initiation and progression of the disease
- Generation of specific T cell and B cell responses and their expansion, requires professional antigen presenting cells (APCs)
- In PMS diffuse tissue injury is also caused by mechanisms other than the compartmentalised immune response, including degeneration
- Tissue damage leads to release of antigens to the periphery, which primes new immune responses in the lymphoid tissue, followed by the invasion of lymphocytes into the CNS Filippi Nature Rev Primers 2018
Aberrant Effector T Cell Activation
Pathophysiology of MS
- Aberrant effector T cell activation due to an insufficiency in the function of regulatory T (Treg) cells and resistance of CNS specific effector T cells to Treg cell mediated regulation Decreased expression of forkhead box protein P3 (FOXP3) by Treg cells and CD25hi CD127low natural Treg cells (which arise in the thymus and are a separate lineage to induced Treg cells - The most stringent Treg definition : CD3+ CD4+ CD25hi CD127low FoxP3+
- Decreased numbers or deficient regulatory responses have also been suggested for CD46 (a complement regulatory molecule, induces Tr1 cells (FOXP3-) with production of IL-10 a potent anti-inflammatory cytokine), CD39 expressing Treg cells, IFNy expressing Treg cells and follicular Treg cells in blood
- The most widely implicated pro-inflammatory effector T cells are IL17expressing CD4+ T cells (known as T helper 17 cells (TH17 cells)) and CD8+ T cells that might be increased in the periphery and in the CNS
- Antibody independent contribution of B cells
- The expression of the microRNA miR155 and proinflammatory cytokines such as TNF, IL12, IL6, IL23 and IL13, which are involved in TH1 cell and TH17 cell differentiation Filippi Nature Rev Primers 2018
Immune System Dysregulation within CNS in MS
Immune system dysregulation within CNS in MS Meningeal vessel SAS Astrocyte Early disease
- Pial basement membrane Glia limitans CNS parenchyma Soluble mediators recruit immune cells Soluble mediators promote inflammation at distal sites CD8 T cell Perivascular DC or macrophage Perivascular immune cell accumulation Oligodendrocyte
- T cell reactivation Myelin sheath
- Vessel activation T.1 cell IFNY MAIT Po IL-17 10 cell 0 TH17 cell Monocyte GM-CSF O Cerebrospinal fluid Phagocytosis Complement proteins Ependyma B cell Choroid plexus Pericyte- - Microglial cell
- Plasma cell Choroid plexus macrophage
Late Phase and Early Phase Dysregulation
- Late Phase
- The acute episodic infiltration of immune cells is diminished
- Neurodegeneration (mitochondrial dysfunction, extracellular free iron accumulation, loss of myelin trophic support, hypoxia, altered glutamate homeostasis and a pro- inflammatory environment, with possible involvement of cytotoxic factors and complement activation).
- Chronic inflammation is mediated by CNS- compartmentalized inflammation involving meningeal immune cell infiltrates (e.g., B cells) forming lymphoid- like structures and by CNS- resident innate cells Early Phase
- Immune cells enter through the blood-brain barrier (BBB), the subarachnoid space (SAS) and the choroid plexus
- MS relapses are characterized by the infiltration of cells of the innate and adaptive immune systems (CD4+ and CD8+ T cells, B cells and myeloid cells), into the CNS parenchyma with perivascular distribution around post- capillary venules of the BBB, activated microglia and astrocytes (oligodendrocyte injury, demyelination and neuro- axonal injury) Meningeal tertiary lymphoid-like structures promote glia limitans damage and astrocyte dysfunction
- Follicular DC Oligodendrocyte progenitor
- Clonally expanded B cells CCL2 GM-CSF Metabolic stress Y Osteopontin NO
- lonic Glutamate · accumulation RNS % · imbalance Energy deficiency Neuro-axonal and oligodendrocyte damage and death CD4+ T cell CD8+ Antibody Neuron r Degraded - myelin protein Demyelination Capillary ROS Filippi Nature Rev Primers 2018
Immune System Dysregulation Outside the CNS in MS
Immune system dysregulation outside the CNS in MS Periphery Blood circulation CNS Thymus Autoreactive T cells can escape central tolerance and be released into the periphery 0 Lymph node Bidirectional exchange BCR Peripheral tolerance breakdown due to TReg cell defects and/or effector cell resistance may contribute to multiple sclerosis development TCR CD4+T cell 1 Memory B cell CD8+T cell o4ß1 integrin TRed cell Reg Infiltration TH1 cell Peptide- MHC Macrophage T_17 cell Bacteria Goblet cell CD8+ MAIT cell Monocyte 0 Viruses Activated innate immune cell Smoke constituents Autoreactive adaptive immune cells can be activated by molecular mimicry, novel autoantigen, release of sequestered CNS antigen or stimulated by bystander activation Dendrou Nature Rev Immunology 2015 B cell Mucosal surface Autoreactive CD4+T cell
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
