Abnormal Findings in Abdominal Examination
Slides about Abnormal Findings in Abdominal Examination. The Pdf, a university-level document, details the inspection, palpation, and auscultation phases, focusing on peristaltic sounds, friction rubs, and bruits, making it a comprehensive resource for students.
See more40 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Abdominal Examination Overview
Abnormal findings in
Abdominal Examination
DR. Hamdi Al Mutori
Consultant Gastroenterologist
MRCP, FRCP (UK)Abdomin Examination:
- Position of pt:
- flat, at the centre of the bed ...
- Exposure: From Symphesis pubis to Sternum - Inspection:
- Any assymtry in the abdomin, shape of Abdo.
- location of umbillicus: Inverted, flat, Everted
formal
-normal contor: S caphoid
- Symmetrical
- Capitus Medusa- above umbilicus
5
- obstruction of sup. vena cava
below umbilicus
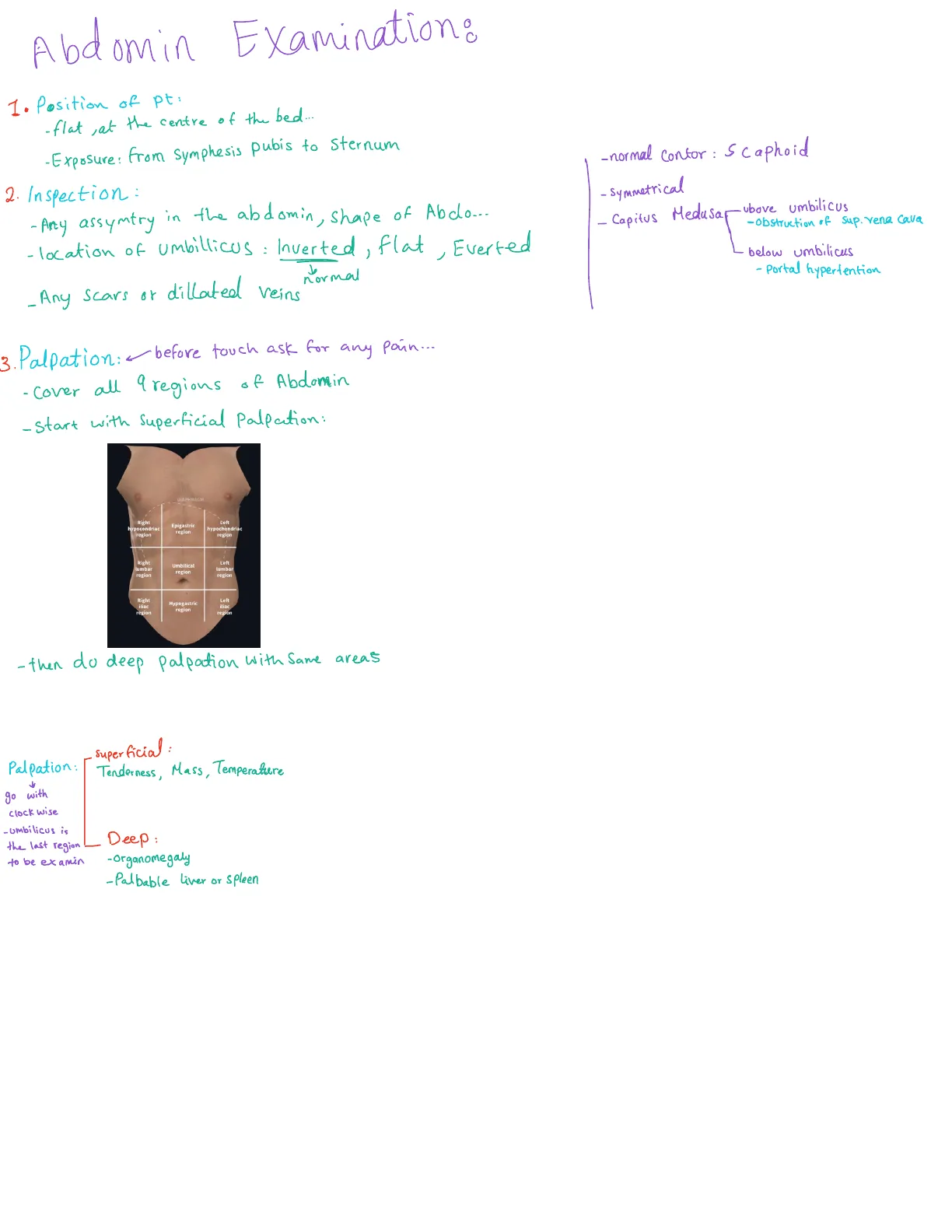
- Portal hypertention - Palpation: - before touch ask for any pain ...
- Cover all 9 regions of Abdomin
- Start with Superficial Palpation:
DIAPHRAGM
Right
Left
hypocondriac
region
Epigastric
region
hypochondriac
region
ITeft
Umbilical
lumbar
lumbar
region
region
region
Right
Left
iliac
Hypogastric
region
region
region
- then do deep palpation with Same areas
Superficial :
Tenderness, Mass, Temperature
Palpation:
go with
clock wise
-umbilicus is
the last region
Deep:
to be examin
- Organomegaly
-Palbable liver or Spleen
- Any scars or dillated veins
Examination of Organs
Liver Examination
RightExamination of organs:
I. liver:
- Right hand flat on abdo ... wall, start from R. illiac fossa with
tip of your fingers more to the R. hypochondrium (fingers parallel to
rectus m. )
- instruct pt to take deep breath
- edge of liver:
upper border:
at 6th intercostal space
where on percasion the sound convert from Resonance
to Dullness
The normal upper level of the liver is at the level of the right nipple, whereas the lower margin of the liver is
at the right costal margin
> measure use tabe 10 cm
Spleen Examination
-Examin the spleen:
from around the umblicas, move diagonally toward left hypochondrium
Cask deep breath, move your hand superficially & Deep, 1cm at bar)
Is you have to palpate along the costal margin as enlargement of spleen could
be variable ...
L, if you can't palpate the spleen, turn the pt on Right side and palpate the Spleen again ...
- if you face any mass: Percuse 2 fingers below or above the mass
then percuss over the mass , to compare b/w
the 2 areas ...
Kidney Examination
Kidney: 2 Kidnies - R & L Side
Put your left hand behind
the back, other hand palpate
the kidney below intercostal margin
آخر
Rec
معلومة
Session Learning Objectives
- Identify abnormal signs on General Physical
Examination - Identify abnormal signs on abdominal inspection
- Identify abnormal signs on abdominal palpation
- Analysis of abdominal mass
- Causes of organomegaly and ascites
- Identify abnormal signs on abdominal percussion
- Identify abnormal signs on abdominal auscultation
General Examination Findings
Patient's General Appearance
General Examination
Note the patient's general appearance
In pain > Peptic ulcer disease (PUD), biliary stone
Altered mental state -> Hepatic encephalopathy
usually present with
Hyperpigmentation of the face > Hemochromatosis-> Chronic liver disease
-
--Nutritional State:
Cachectic/thin ->
GI malignancy, Malabsorption
Well nourished
Obese (truncal or generalized) > risk for gastro intestinal
----
GI
Hands Inspection
Inspect the patient's hands
Clubbing
IBD, Celiac disease, Liver cirrhosis
Iron defesciency anemia
Koilonychias (spoon-shaped nails) > IDA (PUD, Malignancy, Malabsorption)Due to hypoalbunemia
Signs of chronic liver disease > leukonychia (white nails) and palmar erythema,
clubbing, flapping tremor, Dupuytren's contracture.
Eyes Inspection
Cleus in General physical examination
Rec
Inspect the patient's eyes
Pallor -> anemia (GI malignancy, Malabsorption, GI bleeding, chronic illness)
Jaundice ->
Acute or chronic liver disease, cholestasis (Biliary stone, pancreatic tumor)
- Retecular RBCS Count: Prehepatic
KF
Kaiser Fleischer's ring
> Wilson's disease
Wilson's disease is a genetic disorder characterized by
the excess build-up of copper in the body. Symptoms are
typically related to the brain and liver. Liver-related
symptoms include vomiting, weakness, fluid build-up in
the abdomen, swelling of the legs, yellowish skin, and
itchiness.
inflammation
bile duct
Xanthomatous deposits
> Primary biliary cholangitis
Jaundice Causes
In the examination of liver-related issues, the conditions can be categorized into
prehepatic, intrahepatic, and posthepatic causes of jaundice. Here are the main
features associated with each category:
Prehepatic Causes of Jaundice
- Definition **: Conditions that occur before the liver processes bilirubin.
** Typical Causes **: Hemolytic anemia, sickle cell disease, thalassemia. - ** Key Features **:
- Elevated unconjugated (indirect) bilirubin levels.
- Normal or low conjugated (direct) bilirubin levels.
- Increased urine urobilinogen.
- Anemia may be present, depending on the underlying cause.
Intrahepatic Causes of Jaundice
- Definition **: Conditions that affect the liver's ability to process bilirubin.
- ** Typical Causes **: Hepatitis (viral, alcoholic), cirrhosis, liver tumors.
- ** Key Features **:
- Elevated levels of both unconjugated and conjugated bilirubin.
- Possible elevation of liver enzymes (ALT, AST).
- Possible presence of hepatomegaly or splenomegaly.
- Urine may contain bilirubin, indicating conjugated bilirubin in circulation.
Posthepatic Causes of Jaundice
- ** Definition **: Conditions that occur after bilirubin has been processed by the
liver. - ** Typical Causes **: Biliary obstruction (gallstones, tumors), strictures.
- ** Key Features **:
- Elevated conjugated (direct) bilirubin levels.
- Normal or low unconjugated (indirect) bilirubin levels.
- Dark urine (due to bilirubin excretion).
- Pale stools (due to lack of bilirubin reaching the intestines).
Jaundice Summary Table
### Summary Table
Oral Cavity Examination
Examine the patient's oral cavity
Fetor hepaticus -> a distinctive 'mousy' odor of dimethyl sulphide on the breath, which is
evidence of portosystemic shunting (with or without encephalopathy)
Also, Angular Stomatitis
glositis
Signs of IDA -> Angular cheilitis (painful cracks at the corners of the mouth) and atrophic
mascular
glossitis (pale, smooth tongue). The tongue has a beefy, raw appearance in folate and
vitamin B
12
deficiency> Megaloblastic Anemia, Macrocytic anemia
Mouth and throat aphthous ulcers are common in celiac disease and IBD > not specific
most common in ladies:
-bez of Stress
Neck Palpation
Palpate the patient's neck
Gastric and pancreatic cancer may spread to cause enlargement of the left supraclavicular
lymph nodes (Troisier's sign).
More widespread lymphadenopathy with hepatosplenomegaly suggests lymphoma.
Abdominal Examination: Inspection
Inspection Categories
ABDOMINAL EXAMINATION
INSPECTION
(7S)
· Symmetrical & movement with
respiration.
· Scar.
Striae.
· Stoma.
· Shape of the umbilicus (inverted,
flat, exerted).
· Shape of the flank (full, straight,
empty).
· Skin lesions.
(4P)
· Prominent veins (caput medusa,
SVC obstruction)
· Visible Pulsation (aortic
aneurysm).
· Visible Peristalsis (NL in thin,
intestinal obstruction).
· Pigmentation (Cullen's sign,
Gery-Turner's sign)Flat or slightly scaphoid.
Symmetrical => normal shape of
Abdomin ...
Abdominal Distension
Abdominal Acitis, Accumulation of fluid in
the abdominal Cavity
Abdominal distension
If the abdomen is distended, is this generalized or localized?
In obesity, the umbilicus is usually sunken;
In ascites, it is flat or everted.
Look tangentially across the abdomen and fro
bed for any asymmetry associated with a localized mass, such as
an enlarged liver or bladder.
Localized Distension
Localized distension
gall bladder
pick them
GB
on Palpation
Sagoint gall
bladdar
Scars
Scars
for cholesystomy
Kocher
Midline
Laporotomy
Nephrectomy
McBurneys
Pfannenstiel
->Sergical
scar
Mercedes
Scare
9
Liver Transplant
Hernia incision
Striae
Striae
-> diffuse distention of
Abdominal Skin
a major symptoms of
Cushing Synd.Rec
- -. Dilated tertous abdominal wall
RecRey
Surgical Stomas
Surgical stomas
an opening surgically created, which connects a portion of
the body cavity like colon of gastrointestinal tract to the
outside environment
Permenant or Temperorary
STOMa
Bruises and Signs
Bruises. >seve
>sever
1
1
bacterial
bancreatitis
Bluish color at the umbilicus is
Cullen's sign - a sign of bleeding in
the peritoneum.
Bruises on the flanks are Grey
Turner's sign (retroperitoneal
bleeding - e.g. from inflamed
pancreas).
Bruising may also indicate a
bleeding tendency.
Visible Prominent Veins
Visible prominent veins
Usually indicate
intestinal obstruction
Visible Peristalsis
Visible peristalsis
Visible peristalsis is usually
abnormal- a sign of intestinal
obstruction, unless the patient is
emaciated.
Hernias
Hernias
epigastric
umbilical
inguinal
femoral
Abdominal Palpation
Superficial Palpation Observations
Palpation
Observations on superficial palpation
▪
Tenderness : discomfort and resistance to palpation
. Rebound tenderness-when press for while on abdomin,
then remove the press,
Pt will experience sharpe Pain ....
▪
Guarding is voluntary spasm when the physician presses on to the
, take deep breath, Flex his leg
abdominal wall. It is sign of tenderness or inflammation
Rigidity is involuntary spasm (board-like rigidity) Present all the time.
▪
Guarding can often be overcome by having the patient purposely relax the
muscles; rigidity cannot be. Rigidity is thus a clear-cut sign of peritoneal
inflammation.
Gallbladder Tenderness
GALL BLADDER
To feel for gallbladder tenderness
(in cholecystitis):
Murphy's sign
common with pt with
inflammed gall bladar
(cholycestitis)
Abdominal Mass Characteristics
MASS IN ABDOMEN
Site
Size
Shape
Rec
Surface
Consistency-How do feel it? soft , hard, Firm >
Pulsatile
Fixity
)
> to the skin arround it ...
Trans elimination
Tenderness
Temperature
Intraabdominal/abdominal wall ? Rec
Palpable Abdominal Abnormalities
Palpable abnormalities in the abdomen
Epigastric mass
· Gastric cancer
· Pancreatic cancer
· Aortic aneurysm
Hepatomegaly
· Palpable liver not always enlarged
.
· Always percuss upper border
· Palpable gallbladder
Generalised distension
1
· Fluid (ascites)
· Flatus (obstruction/ileus)
· Faeces (constipation)
1
Left upper quadrant mass
· ? Spleen:
Edge
Can't get above it
Moves towards right iliac fossa
on inspiration
Dull percussion note to
9th-11th ribs mid-axillary line
Notch
· ? Kidney:
Rounded
Can get above it
Moves inferiorly on inspiration
Resonant to percussion above it
Ballottable
Tender to palpation
· ? Peritonitis:
Guarding
· Fat (obesity)
1
1
-
-
-
Rebound
Absent bowel sounds
Rigidity
· ? Obstruction:
Enlarged Organs
Enlarged organspt with RHF - will have pulsatile liver
Hepatic enlargement
Chronic parenchymal liver disease
. Alcoholic liver disease
· Hepatic steatosis
· Autoimmune hepatitis
· Viral hepatitis
· Primary biliary cirrhosis
Malignancy
. Primary hepatocellular cancer
. Secondary metastatic cancer
Right heart failure
. -
Haematological disorders
· Lymphoma
· Myelofibrosis
· Leukaemia
· Polycythaemia
Rarities
· Amyloidosis
· Sarcoidosis
. Budd-Chiari syndrome
· Glycogen storage disorders
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
