The Roots of Disease III: Metabolic, Hemostasis and Thrombocytopenia
Document from University about The Roots of Disease III – Metabolic. The Pdf explores hemostasis, coagulation mechanisms, and hereditary thrombocytopenia, including congenital amegakaryocytic thrombocytopenia (CAMT) and its predisposition to bone marrow aplasia. This University document, produced for Biology, details the role of blood vessels in hemostasis and the formation of the platelet plug.
See more48 Pages

Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
HEMOSTASIS
The word haemostasis derives from the Greek and it means "to stop the blood flow", it's the process of forming clots in the wall of damaged blood vessels & preventing blood loss while maintaining blood in a fluid state within the vascular system.
Defects in the haemostasis can lead to an in increasing risk of bleeding (haemorrhage) or clotting (the formation of thrombi). There are three main haemostatic components:
HEMOSTATIC COMPONENTS
- EXTRAVASCULAR: (tissues surrounding the blood vessels) is involved directly in Haemostasis when local vessel is injured. It plays a part in haemostasis by providing back pressure on the injured vessel through swelling and trapping of escaped blood.
- VASCULAR: (The blood vessels through which blood flow) it depends on the size and amount of smooth muscle within their walls and integrity of the endothelial cell lining.
- INTRAVASCULAR: (The platelets and plasma proteins that circulate in the blood vessels). These components are involved in coagulation (clots or thrombus formation) or fibrinolysis (the dissolution of the clot).
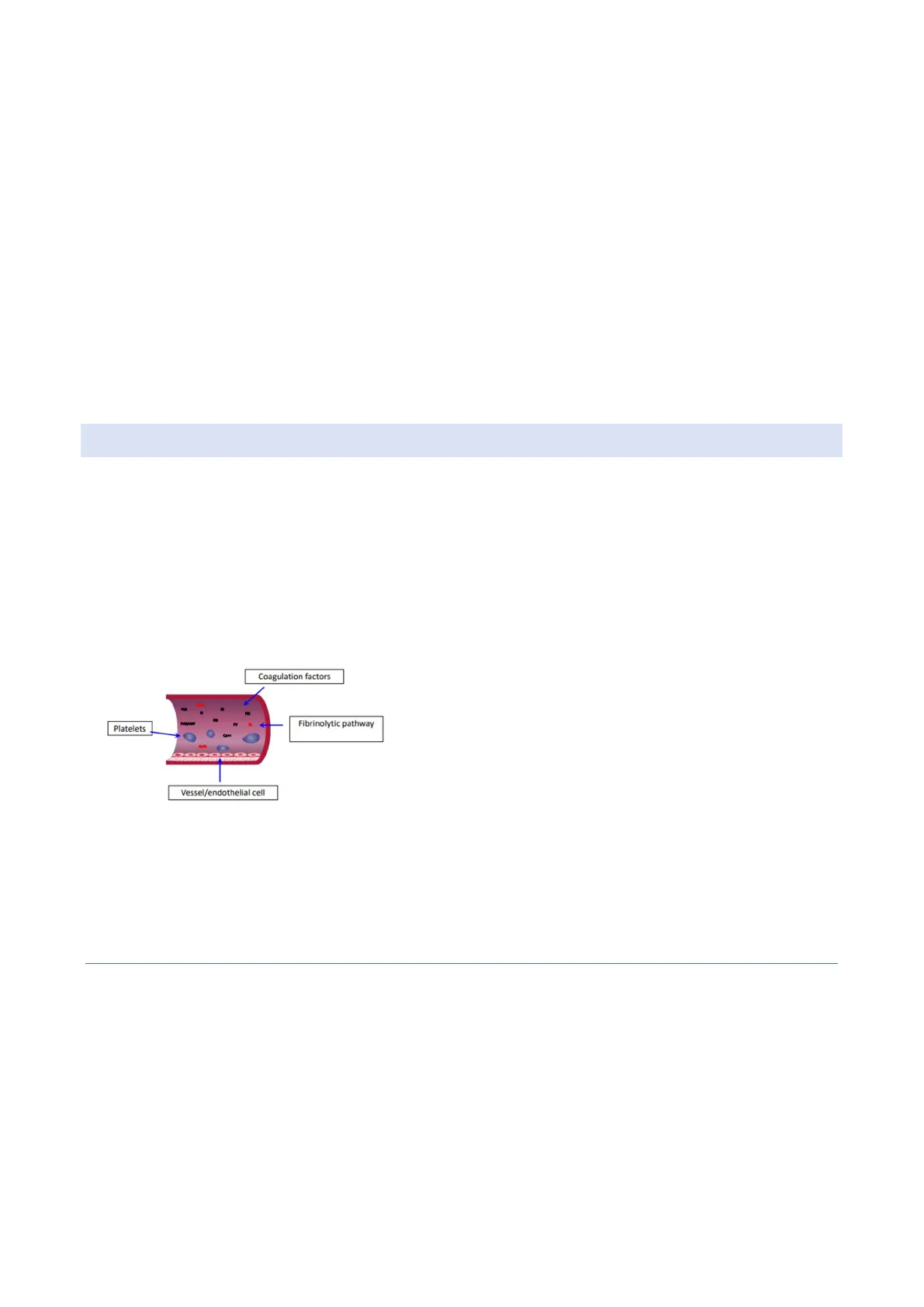
Coagulation factors Platelets Fibrinolytic pathway Vessel/endothelial cell Referred to the image shown: epithelial cells, smooth muscles, platelets, coagulation factors and fibrinolytic pathway. Each component, if injured (primarily or secondarily) results in an unbalance in terms of haemostasis.
In normal conditions, the formation and the dissolution of thrombi it's maintained in a delicate HEMOSTATIC BALACE, without it, patients may experience either excessive bleeding (poor clot formation or excessive Fibrinolysis) or vase occlusion (uncontrolled formation of thrombin in vascular system, occluding vessels and depriving organs of blood).
PRIMARY AND SECONDARY HAEMOSTASIS
Hemostasis can be divided into two stages
- Primary haemostasis: includes platelets and vascular response to vessel injury.
- Secondary haemostasis: includes coagulations factors (plasma proteins) response to such injury.
Together, platelets, vessels, and coagulation factors combine to stop bleeding and allow for vessel repair through formation of a stable fibrin platelet plug at the site of injury.THE HAEMOSTATIC STEPS ARE: (TO KNOW BY HEART FOR THE EXAM)
- Vascular injury
- Contraction of the injured blood vessels
- Platelets adhesion to exposed sub-endothelium collagen
- Shape changes in platelets. They changed their shape from discoidal to spherical with spiny protuberance formation that help the aggregation of the platelets, forming a first haemostatic plug. (they adhere, activate and aggregate forming the haemostatic plug)
- This leads to the local activation of all the processes that determine the conversion of fibrinogen in fibrin, which is deposited locally on the guide of the platelets plug. The platelets form a white clot and then coagulation factors form a red clot, which is stronger than the white one
- Clot consolidation
- Clot remodelling and dissolution through fibrin digestion with complete repair of the vascular wall
PRIMARY HEMOSTASIS
THE ROLE OF BLOOD VESSELS IN HAEMOSTASIS
Blood flows through the vascular system (capillaries, arteries, veins) to and from all the parts of the body. Blood normally is carried within vessels, whose physical capabilities include contraction and dilation, which are controlled by the smooth muscle of the vessel.
Vasoconstriction and vasodilatation provide the means for control blood flow rate and blood pressure. Substances released from the endothelial cells and sub endothelial smooth muscles also contribute to normal blood flow and prevent abnormal formation of clot
CONSTRICTION OF THE VESSEL AND FORMATION OF THE PLATELET PLUG
- The first step of haemostatic process is the vessels constriction, that is translated into a reduction of the blood flow, that allows an increased interaction between platelets with the component of the vessel wall (sub-endothelium collagen)
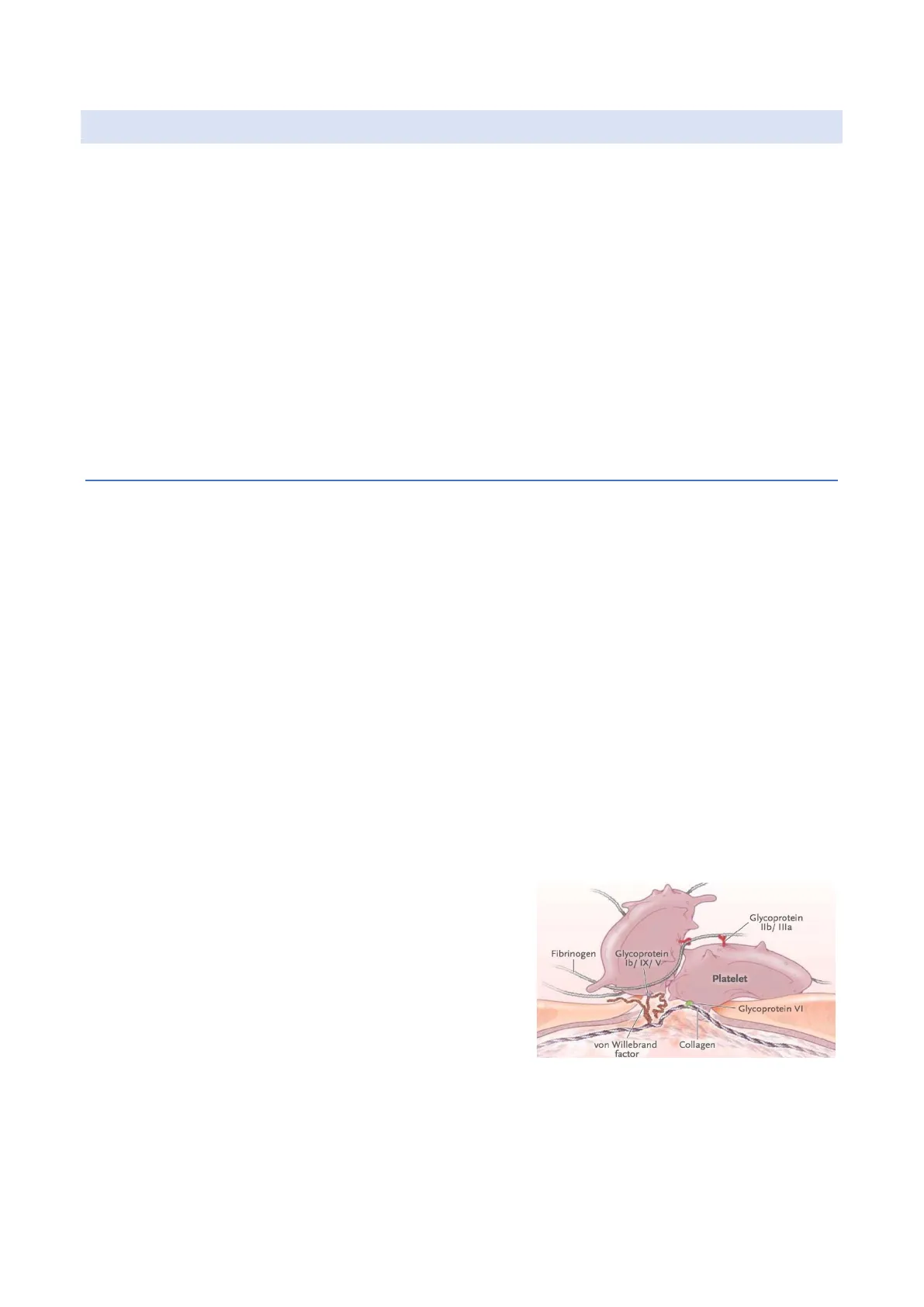
- Then there is the formation of the platelet plug. I. Platelets adhere to the sub-endothelium thanks to the protuberance made by glycoproteins and each glycoprotein complexes with another and can interface and bind to different substrates. During the platelet adhesion the major complexes we are dealing with are vWF/GPIb IX V interaction, collagen/GPIa IIa/GPVI interaction. Glycoprotein Ilb/ Illa Fibrinogen Glycoprotein lb/ IX/ V> Platelet Glycoprotein VI von Willebrand factor Collagen
- Then follows the Platelet activation: influx of calcium, extrusion of platelet storage granule contents, further activation of platelets, irreversible platelet-platelet aggregation (fibrinogen/GPIIb IIIa interaction), formation of the platelet plug and transformation of platelet surface into a phospholipid platform appropriate to support the enzymatic reaction of secondary haemostasis.
PLATELETS ARE ACTIVATED THANKS TO THE INFLUX OF SOME ELECTROLYTES (MOST OF ALL CALCIUM)
FORMATION OF A TIGHTLY PACKED HEMOSTATIC PLUG THAT ARRESTS BLOOD LEAKAGE
Platelets adhere to site of vascular injury Neutrophil Red blood cell Platelet Endothelial cell 0 Basement membrane Collagen and ECM proteins Smooth muscle cell GPIb Inside platelets are presents lots of granules - alpha and delta granules - that are fulfilled of ADP and collagen II. When platelets are activated, they degranulate and release all these substances that can increase again and again the adhesion and the D activation of the platelets (like a circle). This activation leads to the aggregation (one platelet to another), together with all the complexes discussed before, but most of all with the complex GP IIB IIIA. Thanks to the activation and aggregation of platelets, we will reach the formation of the white clot The aggregation and the activation recall and activate the SECONDARY HAEMOSTASIS: the coagulation cascade.
We will see that these complexes are involved in some inherited thrombocytopenias or inherited platelets disorders in which the expression of these complexes is decreased, so it translates into bleeding manifestations, and other typical characteristics that we will see.
On the slide in shown an immunofluorescence image of some platelets: GP1B is a platelet specific marker [] autoantibodies that can recognize GP1B to see how platelets behave during a stress test, or in case of an injury of the vessel.
SECONDARY HEMOSTASIS
The coagulation cascade involves plasma proteins, there are produced in inactivated form and then some enzymes cleave these proteins making them activated. There are two pathways (intrinsic pathway and extrinsic pathway that merge together into a common pathway) resulting in the activation of the fibrinogen in fibrin and the formation of fibrin clots. Coagulation Cascade Intrinsic pathway XII XI VII IX VIII Common pathway Prothrombin Time V Ca++ Lipids The FORMATION OF FIBRIN CLOT works thanks to the exposure to tissue factors present in the sub Į Prothrombin (II) - Thrombin endothelium of vessels cells that are usually hidden from Fibrinogen (I) - Fibrin clot (XIII) blood elements. After an injury, the sub-endothelium exposes tissue factors that activate the coagulation cascade, until the formation of fibrin strand and of a haemostatic clot. The first actor dealing with tissue factors is factor VII (also involves in several bleeding pathologies) that activates the V factor > III factor > | factor > prothrombin -> thrombin > fibrinogen > fibrin. GPIb Platelet aggregation and activation Haemostatic plug formation Activation of coagulation cascade Thromboxane A2 Thrombin Fibrin ADP-0 CD63 C Extrinsic pathway Tissue factor aPartial Thromoboplastin Time
In order to reach a STABLE CLOT, we need another factor that we don't find in the coagulation cascade that is factor XIII that make the clot stable much as possible. Thrombin activates F XIII which covalently crosslinks fibrin strands to form a stable clot which will be retained long enough for vessel repair to occur.
A blood clot can dissolute, coming back to its normal balanced state thanks to the fibrinolytic pathway because this system does not allow the fibrin clot to grow and block a vessel. A blood clot can either continue to grow; in this case it can obstruct the vessel, blocking the blood flow Causing serious complications (deep vein thrombosis). The dissolution of a clot, called fibrinolysis (dissolving of fibrin fibers), is brought about by the formation of the active enzyme plasmin from plasminogen.
Summarizing, haemostasis is dependent upon:
- Vessel blood integrity
- Number and functioning of the platelets.
- Levels and functions of coagulation factors
- Levels and function of fibrinolytic pathway
HAEMOSTASIS IS ORGANISED IN THREE MAIN STAGES:
The main disorders in haemostasis are associated in:
- Initiation: disorders of primary haemostasis
- Propagation: disorders of secondary haemostasis
- Maintenance of blood clot: disorders of stabilization (improper processing and cross-linking of fibrin strands -factors XIII) or problems in the fibrinolytic pathway
If there is an unbalance in the pro-thrombotic factors or anticoagulation factors, we will face a bleeding diathesis or a thrombophilic diathesis. BLEEDING DIATHESIS: spontaneous bleeding or bleeding episodes that are not proportionated to the cause that provokes the bleeding.
Foto slide: Petechiae: cutaneous and superficial bleeding, typical of platelets function disorders. Ecchymosis (or, if profound, haematoma): involves the secondary haemostasis
DISORDERS OF PRIMARY HEMOSTASIS
If we are dealing with primary haemostasis ([2] platelets) what we see in patients are bruising, ecchymosis, telangiectasia, bleeding, menorrhagia for women. For what concerns secondary haemostasis, we observe delaying of haematomas (sometimes it can be a life-threatening condition). For fibrinolytic alteration we observe delayed bleeding or poor wound healing.
Pathway Major component Salient clinical features Classic disorders Primary hemostasis Blood vessel Platelets VWF Bruising Ecchymoses Oozing from mucosa Teleangectasia HTT, vWD Trombocytopenia Dysfunctional platelets Secondary hemostasis Clotting proteins Fibrinogen Delayed hematomas Hemophilia A and B Vitamin K deficiency Liver disease Fibrinolysis tPA a2-plasmin inhibitor PAI-1 Delayed bleeding Poor wound healing Dysfibrinogenemia a2-plasmin inhibitor Liver disease
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
