Pathophysiological Factors Affecting Pharmacokinetics in Renal and Hepatic Disorders
Slides from University of Portsmouth about Pathophysiological Factors Affecting Pharmacokinetics. The Pdf explores how renal and hepatic disorders influence drug behavior, including absorption, distribution, metabolism, and elimination, with an example on pain management in liver impairment. This University level Biology material is ideal for students.
See more12 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Learning outcome
- Describe the major effects of the following clinical states on the pharmacokinetic behaviour of drugs:
- Renal disorders
- Hepatic disorders
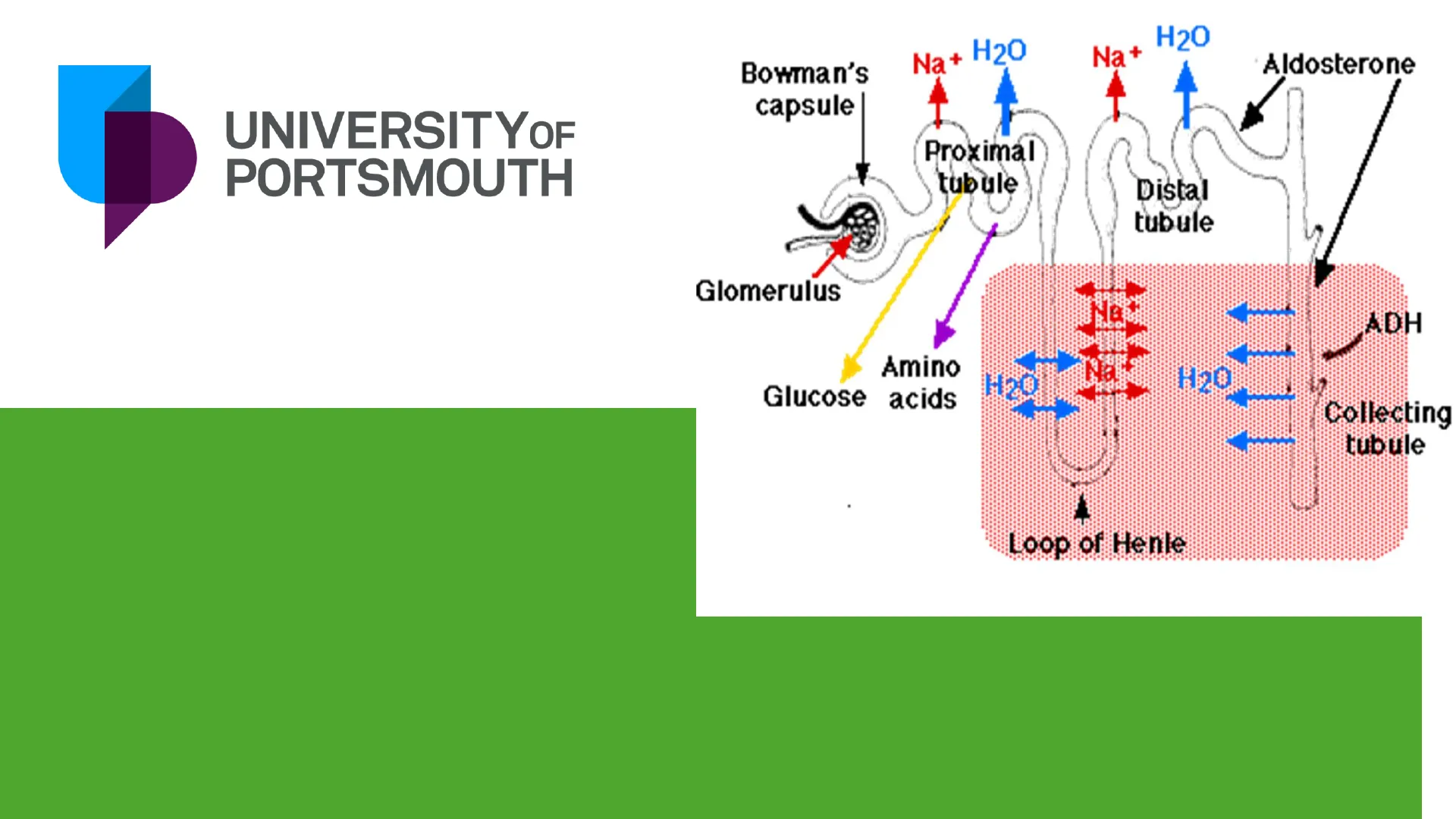
Na + H20
Na +
Aldosterone
Bowman's
capsule
Proximal
tubule
Distal
tubule
Glomerulus
888
ADH
Amino
Glucose acids
H2O
Collecting
tubule
Loop of Henle
1
UNIVERSITYOF
PORTSMOUTH
Renal disorders
Absorption in Renal Disorders
- little specific information
(or apparent clinical significance) - ARF / AKI:
- vomiting (& diarrhoea)
- CRF / CKI:
- Drug/drug interaction - antacids, phosphate
binders interfere (Ca++, other metal++ )
Distribution in Renal Disorders
- reduced protein binding (\ Cpbound)= ^
free drug - displacement and/or low protein levels
- uraemia, hypoproteinaemia both can occur
- total level underestimates free drug
(phenytoin) - More free drug = more available for
Exerting effect
Distributing
Eliminating
Metabolising
Distribution: Oedema and Drug Activity
- oedema
1 Vd (water soluble drugs) - tissue displacement
v Vd (digoxin) - increased activity of some drugs in CNS due to
increased levels of "waste" - increased permeability of BBB
- increased sensitivity - barbiturate, benzodiazepine,
opiate, phenothiazine
Schematic Representation of Protein Binding
Pharmacologic effect
and clearance
. Free drug
Protein-bound drug
Protein-bound molecules
are not available to exert
pharmacologic effects
Metabolism in Renal Disorders
- renal metabolism rarely significant, except insulin
- 25 hydroxycholecalciferol activation to 1,25 dihydroxycholecalciferol (vitamin D)
- (EPO production)
Excretion in Renal Disorders
- primary importance for many
drugs/metabolites - adjust dose or interval for renal
excreted drugs - guidelines based on CrCl
- BNF
- Datasheet/SPC
- Specialist renal textbooks
- increase monitoring
Renal Replacement Therapy
- Effects on drugs vary, partially predictable.
Specialist dose guidelines exist. - Haemodialysis
(diffusion - rapid, intermittent, Mw<500) - Haemofiltration
(filter - slow, continuous, removes higher Mw) - Continuous Ambulatory Peritoneal Dialysis
(CAPD)
(diffusion; peritoneal membrane - slow/ v slow,
continuous, usually small effect on drugs)
Haemodialysis Characteristics
- Rapid removal of low Mw
compounds - (urea, creatinine, electrolytes).
- Around 4hrs, about 3x weekly
- Very rapid drops during session,
gradual rise afterwards - Protein binding, Vd, Mw
- highly bound, large Vd or large
size "not" dialysed - If removed, consider
replacement after session
Haemofiltration Characteristics
- Mostly filtration - less efficient than
dialysis - Replace all lost plasma with salt
solution - "Gentler" process - safer in
unstable patient - Removes most drugs, except v large
- Assume GFR approx 15ml/min
- Haemodiafiltration - combination of
the 2
UNIVERSITYOF
PORTSMOUTH
Hepatic disorders
Liver
Right hepatic
duct
Left hepatic
duct
Hepatic
portal vein
Spleen
Common
hepatic duct
Hepatic
artery
Gallbladder
Stomach
Cystic duct-
Pancreas
Duodenum
(first past of
small intestine)
Common
bile duct
Absorption in Hepatic Disorders
- Absorption of fat-soluble
drugs / nutrients reduced
in cholestasis - Bioavailability may be
increased - reduced 1st pass
metabolism - E.g. if only 10% of your
drug normally gets
through, a small reduction
in 1st pass would DOUBLE
systemic availability - reduced enzyme activity
- portal-systemic bypass /
shunting (advanced
cirrhosis)
Distribution in Hepatic Disorders
- Ascites can alter total body water
- Possibly worsened by drugs
- NSAID's, sodium containing antacids
- Reduced protein binding (less protein
made) - Affects highly protein bound drugs as the
unbound fraction is increased, so
interpreting levels is difficult. e.g.
phenytoin
Ascites is the
accumulation of
fluid within the
abdominal cavity
Schematic Representation of Protein Binding and Pharmacologic Effect
Pharmacologic effect
and clearance
Free drug
Protein-bound drug
Protein-bound molecules
are not available to exert
pharmacologic effects
Metabolism in Hepatic Disorders
- Metabolic capacity of liver generally large
- unless severe hepatic dysfunction
- Depends on individual drug & disease
type (alcoholic liver disease = high
metabolism
... until very small proportion of cells
remain) - Monitor drugs if narrow therapeutic range
- LFT's NOT a measure of enzyme function,
just level of leakage x number of liver cells
(many slightly leaky cells = few very leaky
cells)
Drug Extraction in Hepatic Disorders
- High extraction drugs ("flow
limited") - "unlimited" enzyme capacity -
limited by delivery - 1st pass metabolism
- e.g. chlormethiazole, verapamil,
propranolol - Low/variable extraction
(capacity limited ) - Either limited enzyme capacity
exists for that drug or amount of
free drug present is small (protein
binding)
Cirrhosis and Drug Metabolism
- Alcohol, drugs, viral hepatitis, toxins
- Widespread necrosis / patchy
regrowth, diffuse fibrosis, nodules - Reduced flow through liver, shunting
of blood - Affects phase I metabolism rather
than phase II
(i.e. Oxidation / Reduction /
Hydrolysis more than Conjugation) - Even flow rate limited drugs may be
affected if severe (i.e. "loss" of large
% of cells)
Other Factors in Hepatic Disorders
- Synthesis of clotting factors
- impaired vit K absorption and reduced
capacity - increased sensitivity to anticoagulants
- warfarin, heparin, (aspirin)
- increased risk if drugs can cause bleeding
- NSAID's (aspirin)
- Removal of "toxic" substances
- Nitrogenous substances from gut (1st pass
removal) - If not removed, enter CNS > hepatic
encephalopathy - Also, avoid/care with sedative or CNS toxic
drugs - opioids, benzodiazepines, tricyclics,
(antihistamines)
Example: Pain Management in Liver Impairment
- Mr A, 59 year old (M), 100kg
- Background - decompensated liver
disease (cirrhosis) with ascites.
Analgesic Choice for Mr A
Q. Which ONE of the
following analgesics can be
used for Mr A?
a) Ibuprofen
b) Morphine
c) Paracetamol
d) None of the above
e) All of the above
Pharmacokinetics of Drugs in Liver Disease
PK of the following
drugs in liver disease?
. Absorption - ? fat-soluble drugs
. Distribution - ? protein binding %,
. Metabolism - 1st pass effect, CYP
enzymes
. Elimination - biliary excretion
+ Adverse Drug Reactions?
i.e.) GI bleed. Electrolyte disturbances,
renal impairment, constipation etc ...
+ Hepatotoxicity?
Ibuprofen vs Morphine vs Paracetamol Comparison
- Ibuprofen
- Lipid soluble
- Protein binding
(99%)
- Extensively
metabolised via
liver
- ADRs?
o GI bleed
o Renal impairment
o Hepatotoxicity
o
Fluid retention - Morphine
- Low protein
binding
- Extensively
metabolised via
liver
- Excreted via
biliary system
- ADRs?
o
Sedation
o Respiratory depression
o
constipation - Paracetamol
- Hepatotoxicity in
overdose
(?dose in decomp
cirrhosis)
Summary of Hepatic Disorders
- normal physiological functions of liver affected (alter kinetics or toxicity of drugs)
- intrinsic capacity of liver may be impaired
- first pass metabolism may be reduced
- liver perfusion may be reduced
- reduce dose of liver metabolised drugs
- cholestasis can affect absorption & clearance
- may also have some renal dysfunction
- avoid hepatotoxic drugs or those that worsen existing imbalance
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
