Pulmonary Embolism and Pulmonary Arterial Hypertension Notes
Document from Prof. Coppola about Pulmonary Embolism and Pulmonary Arterial Hypertension. The Pdf explores epidemiology, diagnostic methods like lung scintigraphy, pulmonary angiography, MRI, echocardiography, and compression ultrasonography. This university-level material is well-structured and self-explanatory.
See more20 Pages

Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Introduction to Pulmonary Embolism and Pulmonary Arterial Hypertension
Today we will see two big arguments in respiratory medicine, which are Pulmonary Embolism and Pulmonary Arterial Hypertension. These two major arguments, that maybe you will meet during your professional life, for example, you perform some emergency specialties, or surgery, or Internal Medicine, because as we can see now pulmonary embolism could be a common complication of a lot of other medical conditions. Take care of this argument because, as you know, the vast majority of the questions for example of the written exam (the written part of the exam) insist on the program of the lesson.
Pulmonary Embolism Overview
Brief Introduction to Pulmonary Embolism
Pulmonary embolism represents the so-called "Silent Killer" because nowadays, even if we have reached a modern diagnostic tool to recognize and suspect pulmonary embolism, it still remains vast and largely undiagnosed. This is an example of a big thrombus at the level of the origin of left and right pulmonary arteries, of course, in presence of this kind of thrombus, the subject generally dies.
Outlines and Epidemiology of Pulmonary Embolism
The outline of the argument is quite a remark of the importance of this aspect in Respiratory Medicine, because as you can see, despite the recent advances in prevention and diagnostics, Pulmonary Embolism remains a major health problem, which affects 1/1000 per year in the general population (one per thousand means that in a population like Rome, every year, we have an incidence of more than 3 thousand cases of Pulmonary Embolism). The early diagnosis in this argument is particularly important because the effectiveness of the treatment depends on the time of the diagnosis. Look at the percentages of death every year in the USA: it is around one hundred thousand (from the slides -last year -: Due to the low specificity of its clinical presentation, > 100000 deaths/year in the USA). Although the early treatment is highly effective, Pulmonary Embolism is underdiagnosed. That's why it remains a major health problem and a lead cause of mortality. Now that we go deep in the argument, we will effort (maybe he meant see) two kinds of ways of reasoning about this diagnosis. We will speak about the negative predictive value of a test, and we spoke of the positive predictive value of a test. You have performed Physics and Statistics in the 1st or 2nd year. Does somebody remember what is Negative Predictive Value or Positive Predictive Value? Negative predictive value means that a test can exclude a diagnosis; instead, the Positive Predictive Value of a test means that the test can confirm or suggest the presence of a diagnosis. They are two different ways to approach a problem, but very often when during the workout of the diagnosis of Pulmonary Embolism, generally we have to request additional testing to confirm our suspicions. The venous thromboembolism which is the clinical presentation of the deep vein thrombosis of the pulmonary embolism remains the third most frequent acute cardiovascular syndrome, and if we take in mind that the venous thromboembolism represents the major causes of pulmonary embolism, the suspect of this diagnosis may lead in your mind, every time that you have to check for example the presence of the differential diagnosis of sudden death, dyspnea, syncope. We have performed a few years ago a large European study in a total population, as you can see, of 454 million people, and in Europe, according to this population, we found 370000 deaths. 34% died suddenly, but when we stratify the remnant, only 7% of patients who died were correctly diagnosed. This is the problem, because in a certain sense pulmonary embolism remains a critical event, but this proportion of death is of course over present because we arrive very late in performing diagnosis, because this study says to us that only 7% of patients who die were correctly diagnosed, it means that 93% of patients who die for pulmonary embolism die for an unknown diagnosis and we didn't perform a diagnosis after.
Pulmonary Circulation Characteristics
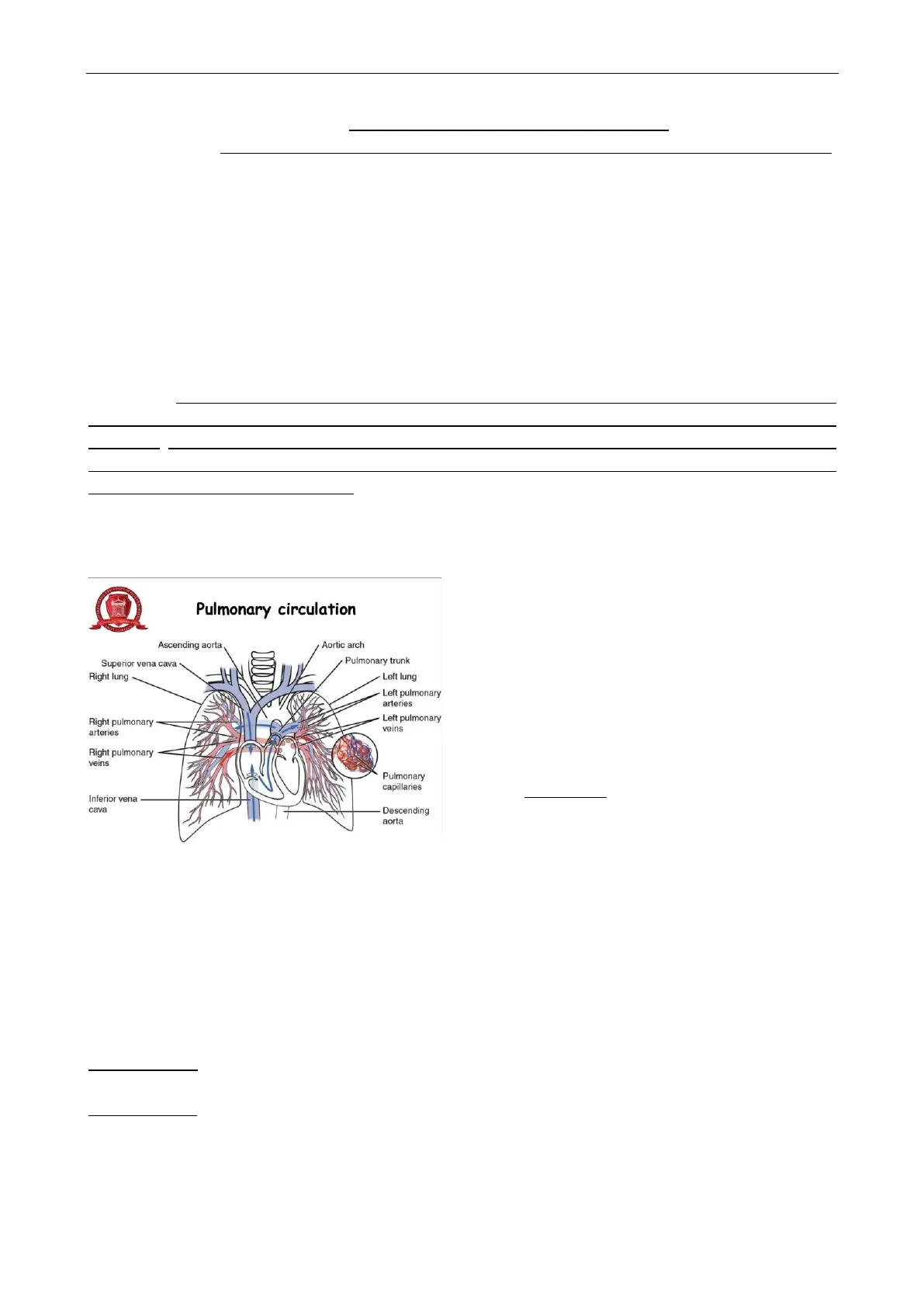
Do you remember from the course of Anatomy and Physiology the characteristics of pulmonary circulation? What does it mean that the pulmonary circulation is double, what it means "the lungs receive a double circulation"? Because of course, the lungs receive the pulmonary circulation with the blood which derives from the right ventriculus, but also the lungs receive the systemic circulation from, above all, the bronchial arteries. Remember: the bronchial arteries derive generally directly from the aorta, that's why sometimes pulmonary hemoptysis or lesion of the bronchial artery may be lethal, very fast, for example in cancer, in tuberculosis. But this belongs to the systemic circulation. The pulmonary circulation depends on the right ventricle and of course, the right ventricle pumps the deoxygenated blood in the pulmonary truncus, and then the pulmonary truncus dividing into two branches (the left and right pulmonary arteries), and then pulmonary circulation which arrives at the pulmonary capillaries and then pulmonary veins, and then left atrium. Do you remember which is the characteristic of pulmonary circulation? Which is the major difference between pulmonary and systemic circulation? The pressure for example is higher or lower in the lung? For example, the normal arterial pressure is around ...? A student answers 93. Professor says: Generally, the normal arterial pressure is 120/80 millimeters of mercury. Do you think that the pressure of the pulmonary circulation is higher or lower? A student replies Lower. Professor says: Of course, it's lower, because the lung is quite at the same level as the heart, but above all, because the pulmonary vascular bed is extremely large, and the blood can perfuse the lung very slowly, that's why the right ventricle does not need to produce high pressure. The right ventricle generally works at very low pressure, around 12-15 millimeters of mercury, 20 millimeters of mercury. Why do I want to underline that? Because we saw, as a complication of the pulmonary embolism, that if I reduce the pulmonary vascular bed, I increase of course the pressure of the right ventricle producing pulmonary arterial hypertension, which is the second argument of today. Keep in mind this simple image because it gives us important information. The vast majority of pulmonary embolism depends on the genesis of emboli from the lower part of the body, first of all, the deep vein thrombosis of the leg, and generally pelvis. The mechanism is quite brutal, simple: I have a thrombus generally in the part in which the blood flux is lower, I have a thrombus. A fragment of this thrombus leaves the thrombus (the name of the fragment is embolus), and the embolus follows the blood flux of the vein. Differently from the artery branch, in which the caliber of the arteries decreases from the heart to the peripheral part, at the level of the veins, we have the opposite: the veins become larger, so the embolus generally does not find any filter and arrives in the right atrium, and then arrives in the right ventricle, and the right ventricle pumps the embolus in the pulmonary branch, and then the embolus stops elsewhere in the pulmonary vascular bed. When the embolus stops a vessel, it produces a pulmonary embolism. Of course, the major is the dimension of the embolus, the major is the damage that the embolus can produce at the level of the lung.
Blood Flow to the Lungs and Clot Travel
The venous system from the upper and lower parts of the body drains into the right atrium, and the right ventricle pumps the blood in the lung, so if a clot occurs in any vein, it will eventually end up in the right side of the heart. The heart then pumps in the pulmonary arteries and the pulmonary arteries become smaller, in that condition we have a different process, overcome, after the embolus passes the truncus, the pulmonary arteries become smaller, and then the blood clot becomes caught in the lung. This is, brutally, the pulmonary embolism from the mechanical point of view.
Typically, there is more flow in the lower area of the lung due to gravity, due to the West zone, that we saw in the Respiratory Failure; and Pulmonary Embolism can occur anywhere, but more are seen in the lower portion of the lung because the flux is higher in that area. No preference of site, differently for example from the bronchi, because generally if you have a foreign body in the trachea, generally it's more common that arrives at the level of the right bronchus because it's shorter, it's larger, and because it starts directly from the trachea. Instead, we have no preference to which site pulmonary embolism occurs at the level of the vessels.
Saddle Embolus
Pay attention to the saddle embolus: the saddle embolus is the embolus that I put as the first image of the lesson. The saddle embolus is terrible because it's a clot that occurs at the point of the pulmonary artery branching, and generally - as you can imagine- a block, a stop at the level of the branching of the pulmonary artery generally is lethal because a large amount of blood is stopped.
V/P Mismatch in Lungs
In the lungs, the blood clot gets lodged in the pulmonary artery, so there is no perfusion, but we have ventilation. Do you remember when we spoke about Respiratory Failure, the VP mismatch (ventilo-perfusion mismatch)? This is a clear example of ventilo-perfusion mismatch. And do you remember the name of this phenomenon when we have ventilation but no perfusion? Shunt or dead space? A student replies to Dead space. The professor says it's correct.
Lung Infarct Consequences
And the other consequence is the lung infarct: there is an increase in resistance of the blood flow which can also produce a cardiac arrest, but the lungs may infarct even if, differently from other tissue, generally if the clot stops the pulmonary circulation, the tissue remains perfused by the pulmonary artery, perfused by the systemic circulation of the bronchial arteries.
Virchow Triad and Thrombosis
The mechanism which underlines the production of thrombosis is linked to the so-called Virchow's Triad (that maybe you have studied in Physiology). The Virchow's Triad remains the most simple, beautiful, and genial description of the genesis of thrombosis, and
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
