Respiratory Physiology: Chronic Obstructive Pulmonary Disease Pathogenesis
Slides about Respiratory Physiology: Chronic Obstructive Pulmonary Disease (COPD) Pathogenesis. The Pdf, a presentation for University Biology students, explores inflammatory mechanisms and airflow limitation in COPD, based on the abstract summary and outline.
See more27 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Chronic Obstructive Pulmonary Disease (COPD)
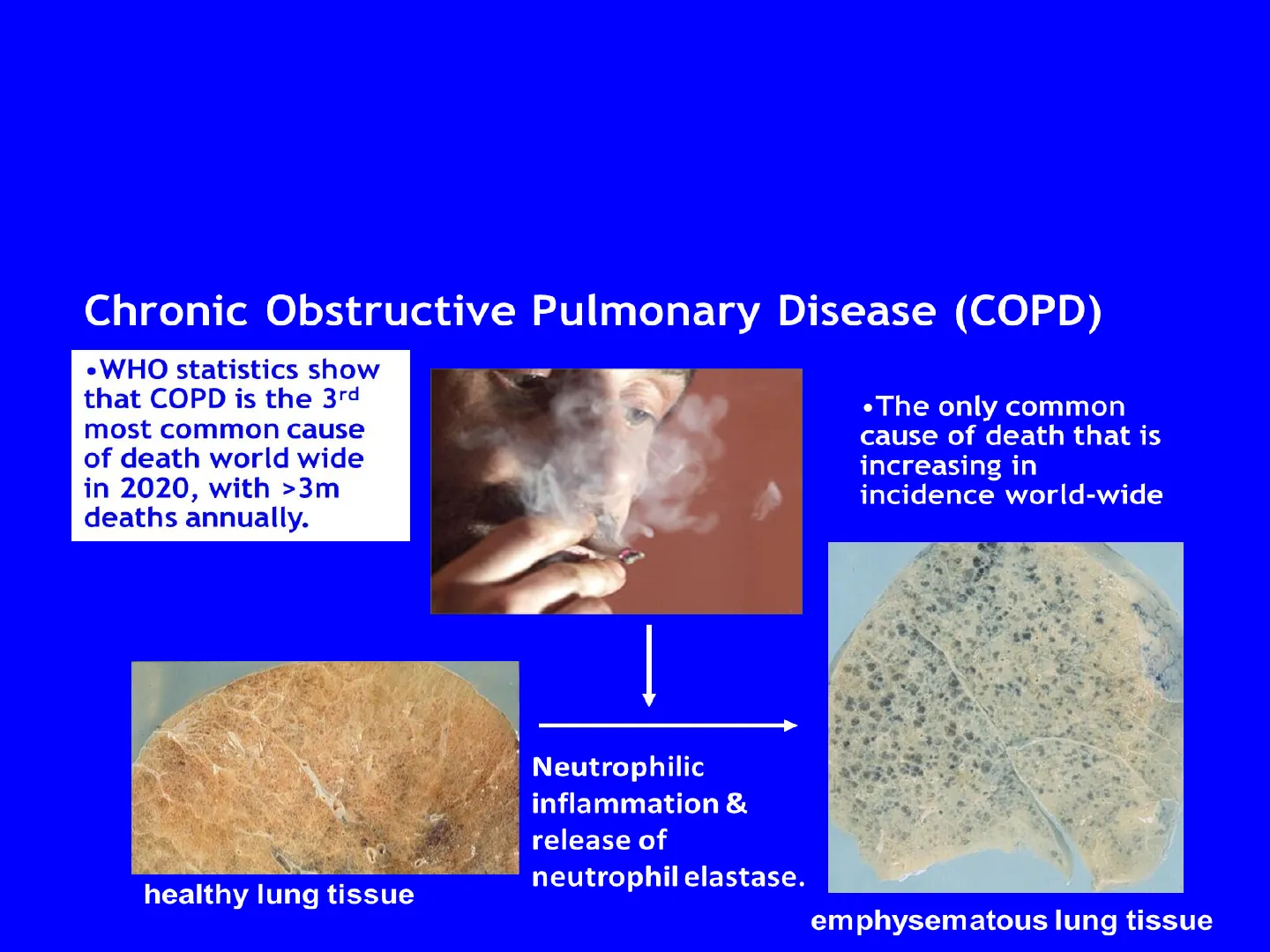
Chronic Obstructive Pulmonary Disease (COPD)
. WHO statistics show
that COPD is the 3rd
most common cause
of death world wide
in 2020, with >3m
deaths annually.
. The only common
cause of death that is
increasing in
incidence world-wide
Neutrophilic
inflammation &
release of
neutrophil elastase.
healthy lung tissue
emphysematous lung tissue
- Chronic obstructive pulmonary disease is commonly known as COPD and is a chronic
inflammatory disease of the lower airways. COPD is strongly associated with smoking, and also
air pollution, occupational exposure to dust and gases and genetic factors. Only 15% of smokers
get COPD, suggesting genetic factors play a role .. In developing countries, cooking indoors
over open fires is a significant risk for developing COPD (see next slide). - Although there are approximately 250 million diagnosed cases of COPD globally, this is likely
to be an underestimate as most COPD is in low-middle income countries where records are not
accurate. Overall, it is estimated to affect 650 million people in the world, based on WHO
estimates that COPD affects 10% of the worlds population, which is 6.5 billion. - The incidence of COPD is increasing. It is the 5th most prevalent disease and 3rd most common
cause of death in 2020. - Smoking stimulates an inflammatory response and the accumulation of neutrophils in the
airway. Neutrophils play a central role in the pathophysiology of the disease. When neutrophils
are activated they release and enzyme called neutrophil elastase that breaks down elastin in the
elastic connective tissue and destroys the alveoli. This reduces the surface area available for gas
exchange and leads to hypoxia-which is insufficient oxygen in the circulation. Normal healthy
dense lung tissue is destroyed irreversibly, this is called emphysema, and reduces lung function
irreversibly. - Some patients have a genetic susceptibility to developing COPD because they have an inherent
deficiency in alpha1-antitrypsin, an important inhibitor of neutrophil elastase found in the
blood. - Macrophages are also present in increased numbers and accumulate particulates from cigarette
smoke. Activated macrophages also release tissue damaging proteases.
COPD in Low-Middle Income Countries
Most COPD is in low-middle income countries
Credit: Photo courtesy of Global Alliance for Clean Cookstoves
In developing countries, cooking indoors over open fires made of wood, peat and animal
dung, and inhaling the smoke particles, is a significant risk for developing COPD.
Understanding Chronic Obstructive Pulmonary Disease
What is chronic obstructive pulmonary disease (COPD)?
- COPD is sometimes called chronic obstructive
airways disease (COAD) - Characterised by progressive development of
airflow obstruction that is irreversible - It is the 4th most common cause of death in the
UK and 3rd in the world - It kills 25,000 people each year in the UK, which
is more than bowel, breast or prostate cancer - There are an estimated 3 million people with
COPD in the UK, although < 1 million are
correctly diagnosed - It is a major health burden on the NHS and
accounts for 10% of all working days lost each
year - It is due to a mixture of emphysema (destruction
of alveolar walls), bronchiolitis (inflammation of
the bronchioles) and chronic bronchitis (mucus
hypersecretion).
COPD is a disease characterised by
irreversible airflow obstruction and
the relentless and progressive loss of
lung function.
The health and economic burden of
COPD is enormous and the
incidence and mortality is increasing
on a world-wide basis. It is
associated with an increase in
cigarette smoking and environmental
pollution in developing countries. In
industrialised countries it is mainly
associated with smoking.
Ischaemic heart disease and stroke
are the world's biggest killers, COPD
is the third most common cause of
death globally.
In the UK leading causes of death
are ischaemic heart disease,
dementia and Alzheimers, lung
cancer and COPD.
Symptoms of COPD
Symptoms of COPD
- key indicators for considering a diagnosis of
COPD
- Wheezing (especially on exercise)
- Breathlessness (dyspnea)
- Cough
- Sputum production
- Recurrent infective exacerbations
Components of COPD
A
Chronic
bronchitis
Small
airways
disease
Emphysema
B
C
SA
SAD
E
Components of COPD.
A: COPD comprises 3 interlinked
conditions, namely, chronic bronchitis
(CB, airway mucus hypersecretion),
small airways disease (SAD, chronic
bronchiolitis), and emphysema (E,
alveolar destruction). The relative
contribution to airway obstruction of
each component in any one patient is
often unclear.
B: Patient in whom mucus
hypersecretion (CB) predominates (may
be identifiable by excessive sputum
production).
C: Patient in whom mucus
hypersecretion contributes proportionally
less to airflow limitation than SAD and E.
- There are three components to COPD;
- Emphysema. Emphysema is the destruction of lung parenchymal
tissue, the enlargement of airspaces, loss of lung elasticity and
closure of the small airways. - Bronchiolitis. Bronchiolitis is inflammation and obstruction of the
small airways. - Bronchitis. Bronchitis is overproduction of mucus in the bronchi
and productive cough. - Usually all three components are present, but the relative
contribution varies in each patient. - COPD is an umbrella term that covers these different pathologies,
irrespective of the contribution of each. Patients are therefore a
very heterogeneous group displaying different symptoms.
COPD Phenotypes: Pink Puffers and Blue Bloaters
Two extreme cases; Pink puffers and Blue bloaters
Pink puffers have predominant emphysema, the onset of disease is
characterised by breathlessness, their general appearance is thin and
emaciated, use purse-lipped breathing, age 50-75 years. Cachexia.
Blue bloaters are generally overweight with peripheral oedema and a
marked cyanotic appearance, due to hypoxia. The onset of disease is
characterised by a prominent cough with copious, often purulent, sputum
as these patients are prone to recurrent chest infection, age 40-45 years
Symptoms of COPD;
Depending on their phenotype, patients may have
- Cough and sputum production for many years
- Infective exacerbations of the disease
- Breathlessness and wheezing, especially on exertion
At the extremes
- 'Blue bloaters' have increasingly severe exacerbations of disease leading to hypoxia with cyanosis, tissue oedema,
muscle weakness, respiratory and heart failure. Hypoxia contributes to muscle weakness and fatigue. - 'Pink puffers' have little or no sputum production or hypoxia at rest, but severe breathlessness and prominent
emphysema. Patients commonly underweight with cachexia and skeletal muscle wasting.
Causes of COPD
What are the causes of COPD;
- SMOKING! The commonest cause, 15% of smokers develop COPD
- Passive smoking is weakly associated with COPD
- Air pollution, particularly with sulphur dioxide and black smoke
particles from cooking indoors in undeveloped countries - Occupational exposure to fumes and dust. Exposure to cadmium is
associated with emphysema
Early exposure to - Chest infection during the first year of life
- Early nutrition, low intake of dietary antioxidant vitamins (A,C & E)
- Genetic factors, such as alpha1-antitrypsin deficiency, lead to
emphysema.
Smoking is the most common cause of COPD in industrialised countries. In
developing countries, environmental pollutants are important causes, for
example smoke from cooking on open fires indoors in confined spaces.
- Tobacco smoke is a mixture of more than 4,700 chemical compounds.
There are 1018 particles in every puff and 1016 free radicals or oxidant
molecules. - Known exposure to risk factors contributes to a diagnosis of COPD.
- Genetic factors are indicated since 15% of white smokers get COPD, but
only 5% of Asian smokers, ie there is a different prevalence between racial
groups. Also, there are clusters of patients within families with COPD.
Polymorphisms in a number of genes have been associated with COPD,
such as a deficiency in the protease inhibitor, 1-anti-trypsin, or an increase
in pro-inflammatory cytokine TNF.
Diagnosing COPD with Spirometry
The diagnosis of COPD, indicated by symptoms and
exposure to risk factors, is confirmed by spirometry
SPIROMETRY - NORMAL TRACE
SPIROMETRY -
OBSTRUCTIVE DISEASE
5
4
FEV1 = 4L
Volume, liters
FVC = 5L
3
FEV1/FVC = 0.8
2
1
0
1
2
3
4
5
6
Time, seconds
5
4
Volume, liters
3
2
FEV1 = 1.8L
FVC = 3.2L
Obstructive
1
FEV1/FVC = 0.56
0
1
2
3
4
5
6
Time, seconds
Symptoms
indicative of
COPD are
confirmed by
spirometry,
and
FEV1/FVC <
0.7
FVC =
FEV1 =
Annual Decline in Airway Function
Annual decline in airway function, showing accelerated decline
in susceptible smokers and effects of smoking cessation
100
GOLD 1
non-smoker
I
I
non-susceptible
75
smoker
GOLD 2
susceptible smoker
- stop smoking, age 50
50
GOLD 3
disability
stop smoking, age 65
GOLD 4
25
death
0
25
50
75
Age (years)
FEV1 (% predicted)
- As we get older there is a normal decline in lung function, but smoking speeds up the rate of
decline in lung function. - COPD is associated with an increased rate of decline in lung function. If a patient with COPD
stops smoking the rate of decline will go back to normal, but they will not get back the lung
function they lost. - Longitudinal monitoring of lung function shows an accelerated decline in lung function in 15% of
smokers who are susceptible. Normal decline in lung function of about 15-30 ml in FEV1 per year,
is increased 2-5 fold in COPD patients to about 80 ml per year. - Stopping smoking is the most beneficial strategy, and to stop smoking at the age of 50 can result in
normal life expectancy, but poor quality of life. - Death is from respiratory failure and hypoxia leading to cardiac failure.
- GOLD is the Global Initiative on Obstructive Lung Disease and has defined the boundaries of lung
function that define disease severity; - GOLD 1=mild disease
- GOLD 2=moderate disease
- GOLD 3=severe disease
- GOLD 4=very severe disease
Classification of Airflow Limitation Severity in COPD
CLASSIFICATION OF AIRFLOW LIMITATION SEVERITY
IN COPD (BASED ON POST-BRONCHODILATOR FEV,)
In patients with FEV1/FVC < 0.70:
GOLD 1:
Mild
FEV, ≥ 80% predicted
GOLD 2:
Moderate
50% ≤ FEV, < 80% predicted
GOLD 3:
Severe
30% ≤ FEV, < 50% predicted
GOLD 4:
Very Severe
FEV1 < 30% predicted
TABLE 2.4
The GOLD number confirms persistent airflow limitation, and indicates
the degree of airflow obstruction and severity of disease.
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
