Neurology: Neurological Examination and Diagnostic Techniques
Document from University about Neurology. The Pdf provides a detailed overview of the neurological examination, covering aspects such as medical history, diagnostic tests (EEG, EMG, evoked potentials), and vegetative functions. This Biology document is useful for university students.
See more50 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Neurology
Neurological Examination 2 Physiology of Sensory and Motor Systems 8 Evoked Potentials and EMG 23 Cranial Nerves 28 45 Autonomic NS Ataxia 50 Headache 52 EEG 60 Epilepsy 65 Multiple Sclerosis 78 93 Dementia 107 Parkinsoninan Syndromes 114 Neuropathies 125 Motor Neuron Diseases 132 Myopathies 141 NMJ Disorders 157 Meningitis 162 Encephalopathies 167 Myelopathies 186 Coma and Consciousness Disorders 193 Symbolic Disorders 198 Sleep Disorders 205 Brain Tumours 208 Page 1 of 214 Cerebrovascular DiseasesNeurological Examination
Neurologist's Tools
Hammer: also equipped with a small pin at the back to test superficial sensations. Diapason: used to assess proprioception, this is an essential information that our brain needs to adjust movements on the bases of how/where we are located.
Neurological pts are typically affected by a chronic condition - they tend to have a long history. Understanding the history might be relevant also for the diagnosis because degenerative conditions might mimic each other at the beginning but, later on the picture gets clearer.
Another feature of these pts is that they may have a cognitive impairment, and history might be taken in collaboration with a caregiver.
The main tests are blood tests and CSF analysis, CSF can give a lot of information about infectious or inflammatory diseases, demyelination or degeneration.
The other tests can be divided into 2 classes:
Neurophysiological Testing
- Electroencephalography (For the CNS)
- Electromyography and electroneurography (for the PNS)
- US of carotid and vertebral arteries
- Evoked potentials, to assess nervous pathways by giving a stimulus at the periphery and registering it in the cortex (somatosensory evoked potential) and vice versa (motor evoked potential)
Imaging Tests
- CT scan and Angio CT
- MR and Angio MR
- Angiography
- Nuclear medicine tests (SPECT and PET)
Some conditions might be diagnosed early based on the history, for instance migraine. In other conditions, neurological examination plays a pivotal role, like in spastic paraparesis, characterised by an increased muscular tone in the lower limbs which loose strength.
With neuroanatomy and physiology knowledge we are able to perform a neurological examination and localise the lesion to know at which level to perform further investigations. In neurology the severity of damage and its location are crucial, because they will lead to different clinical phenomenology and different workups needed.
Clinical History
Clinical History: focus on identifying important information and avoid uninformative elements. Witnesses and caregivers' interviews are crucial in patients with cognitive impairment or that experienced loss of consciousness.
The questions we ask to the patient depend on the nature of symptoms and their localisation. The nature of symptoms can be:
- Negative: a function is lost (e.g. paralysis)
- Positive: hyper-excitability of the system (e.g., pain or clonus* which is a sign of pyramidal tract impairment)
- Peculiar: for example, throbbing headache typical of migraine
*set of involuntary and rhythmic muscular contractions and relaxations, associated with upper motor neuron lesions.
The localisation of symptoms might be:
- Unilateral or bilateral: bilateral symptoms are rarer and usually indicate a lesion in the spinal cord or a nerve involvement. Brain lesions are rarely the cause of bilateral symptoms because only a very big lesion or multiple lesions would cause them.
- Presence of gradient/pattern of progression: lesions might start distally and move proximally. Typical of Guillain Barre syndrome, an autoimmune condition of peripheral nerves
- CNS or PNS involvement
Symptoms might also have a temporal pattern, an hyperacute onset is typically caused by a vascular involvement like a stroke. The onset might also be acute or subacute with progression (Guillain-Barre or infections). Chronic conditions might be fluctuating like in multiple sclerosis, or progressive, typical of neurodegenerative (such as Alzheimer's disease) and neoplastic disorders. The pattern might also be intermittent, in this case we might observe a full recovery in between symptoms.
Many neurological conditions are typical of elderly people and co-morbidities are relevant, especially vascular and heart related ones.
Vegetative functions like sleep, bladder, intestinal and sexual alterations should also be assessed. Social information should be investigated because neurological conditions might be different based on the patients employment. Pharmacological and familiar history are also important and should be considered.
Neurological Examination Features
Neurological examination: the features to be investigated are:
- Vigilance, cognition and mental state
- Cranial nerves
- Motor system: strength, tone and coordination
- Reflexes
- Sensory system
- Balance
- Gait: it's due to many things which need to work properly together.
Vigilance Assessment
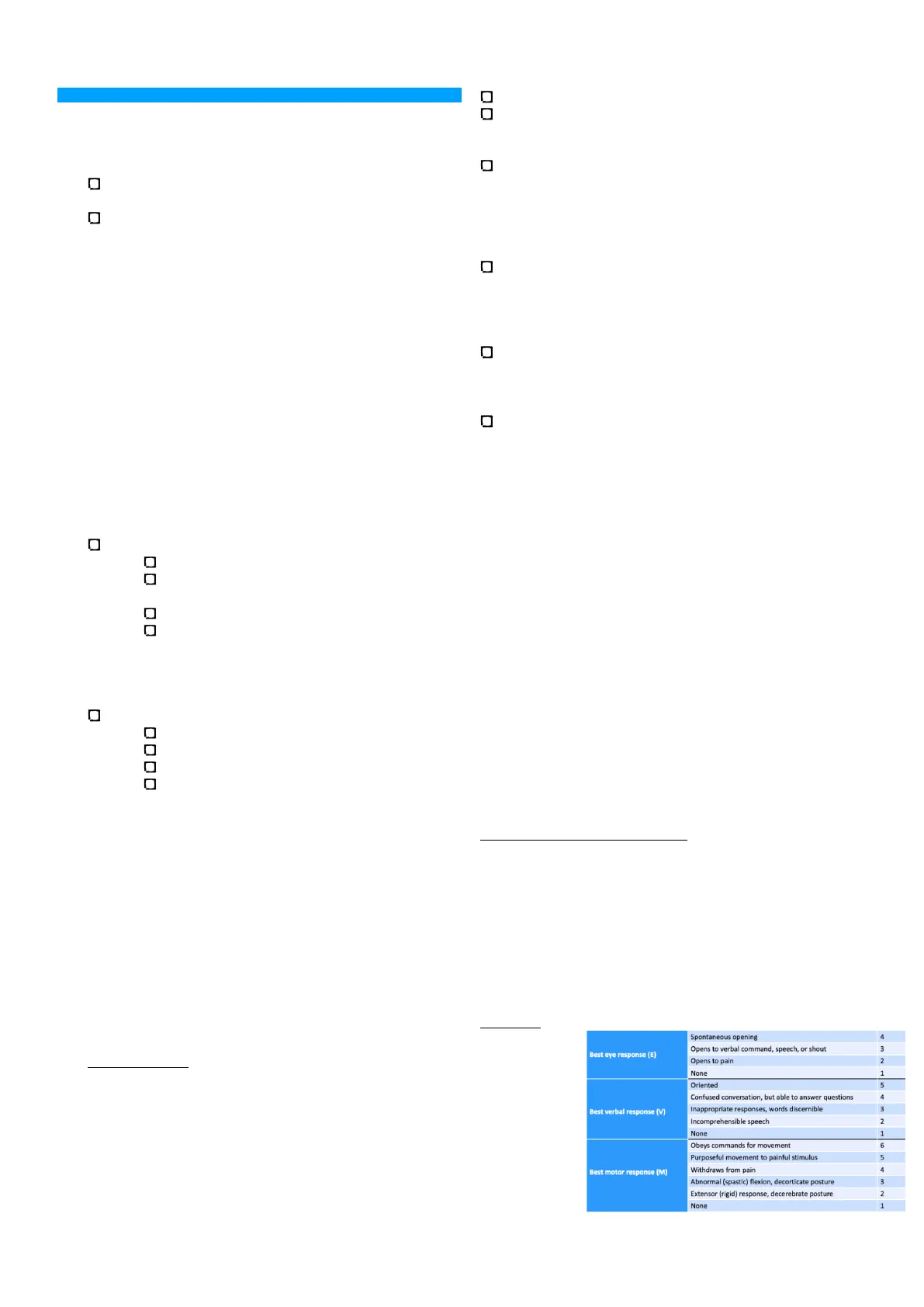
Vigilance: The patient needs to be present enough to perform the exam, a useful scale to assess vigilance is the Glasgow coma scale (GCS) that allows us to rate the Spontaneous opening 4 Opens to verbal command, speech, or shout 3 Best eye response (E) Opens to pain 2 None 1 Oriented 5 Confused conversation, but able to answer questions 4 Inappropriate responses, words discernible 3 Incomprehensible speech 2 None 1 E Purposeful movement to painful stimulus 5 Withdraws from pain 4 Abnormal (spastic) flexion, decorticate posture 3 Extensor (rigid) response, decerebrate posture 2 None 1 1 Page 2 of 214 Best verbal response (V) Obeys commands for movement Best motor response (M)severity of loss in vigilance. We need to test the best eye. verbal and motor responses. For each response we give a score. For example the best eye response is when the patient has a spontaneous eye opening; in other patients, the eyes are closed but after a verbal command, speech or shout he/she opens them. The patient might open their eyes only after a painful stimulation or, in the worst cases, the eyes remain closed. The final total score goes from 3 to 15, the worst possible score is 3 with severe coma. A patient with a score of 15 will have spontaneous eye opening. will be oriented and will obey to commands for movements.
Cognition and Mental State
If the patient is vigilant, we can assess the cognition and mental state. Firstly, we test the orientation with some easy questions such as: "Where are we?" (space) or "What day/year is today?" (time).
To assess the language there are some psychological testings, but we can start to have an idea by asking the denomination of common objects, or by giving simple orders like "raise the right hand". The language requires a symbolic system and not just sounds and it is associated with the production of symbolic sounds. In this way we assess the two main abilities associated to the language which are the ability to produce symbolic sounds or signs and to understand them. If there is a damage to the pathway connecting the understanding and producing part, the patient can understand and produce language but might be unable to repeat sentences.
Another thing we test is ideation, evaluating its contextual appropriateness and processing speed. The patient should behave accordingly to the context. Processing speed is how rapidly the patient can process the information that is given from the environment. A specific phenomenology is associated to a damage in a specific area of the brain with a specific function. A patient with a subcortical pathology, of the fibres connecting the different cognitive areas, has a normal function but at a slower pace.
The mini mental state examination is used to assess different cognitive aspects: orientation in space and time, memory attention, ability to recall words and language.
Every aspect has a score, the maximum score is 30 and it belongs to patients which have a very good state; up to 25-26 is still considered normal. A score below 25 indicates a problem. It's important to correct the final value according to the level of education of the patient.
Cranial Nerves
Cranial Nerves: There are 12 cranial nerves all originating from the brainstem, except for the olfactory and optic nerve, all the nerves are bilateral.
- Olfactory
- Optic
- Oculomotor
- Trochlear
- Trigeminal
- Abducens
- Facial Vestibulocochlear Glossopharyngeal Hypoglossal Vagus Cranial Accessory
- Accessory
- Hypoglossal
The optic nerve is not a nerve, it's a part of the CNS. This is important because myelin surrounding the CNS fibres and the PNS fibres are two different types of myelin. Autoimmune conditions attack the peripheral myelin but not the optic nerve, while central pathologies such as MS will affect the optic nerve but not the peripheral myelin. This phenomenon occurs because the myelin in the CNS is produced by oligodendrocytes while the myelin in PNS is produced by Schwann cells; they are biochemically completely different.
Olfactory Nerve (CN I)
Olfactory (CN I): not usually studied in the classical neurological examination because it's very complicated to test it. We usually ask the patients if they are experiencing a reduced olfactory activity because, apart from flu and COVID, hyposmia in neurology is typically due to Parkinson's disease. We use substances like coffee, vanilla and cinnamon and compare them to a "blank" sample.
The ammonia test is performed because it irritates the CN V people with true anosmia shouldn't feel coffee but they should have an irritation of the trigeminal nerve with ammonia. This would mean that there is not a mucosal damage.
Optic Nerve (CN II)
Optic (CN II): The optic pathways start in the retina. The temporal Left visual field Right visual field retina brings information from the Temporal Nasal contralateral visual field Temporal Optic chiasm and the nasal retina from the ipsilateral visual field. The fibres Pulvinar nucleus and the axons join to Lateral geniculate nucleus Superior colliculus form the optic nerve, they move posteriorly Optic radiation and medially to reach the optic chiasm in which there is the partial decussation of the fibres, only the nasal fibres will decussate. These fibres will form the optic tract and reach the thalamic complex, particularly the lateral geniculate complex (LGB). From the LGB there is the formation of optic radiations, which are located in the posterior part of the brain, to reach the primary visual cortex in the occipital lobe (Brodmann area 17).
Primary visual cortex Along the course of the optic tract, some fibres leave the tract to join the Edinger-Westphal nucleus, which is the parasympathetic component of the CN III. It controls the pupillary light reflex causing miosis in bright light and mydriasis in dim light.
If there is a lesion anteriorly in the optic nerve there will be e complete loss of vision. If the lesion is in the posterior part where optic radiations are open and occupy a very large part of the brain, we would need a very big lesion to impair at least half of the visual field - a small loss and normal pupillary reflexes is likely caused by a posterior lesion while a big one with impairment of pupillary reflexes is caused by an anterior one.
To test visual deficits there are specific ophthalmological tests, we could ask the patient to look at our nose while we move our hands in different parts of their visual field.
Visual acuity can be tested by making the patient read Page 3 of 214 Optic Oculomotor Trigeminal Trochlear Abducens
- Facial
- Vestibulo-cochlear
- Glossopharyngeal
- Vagus
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
