Adaptive Immunity: Primary and Secondary Lymphoid Organs
Slides from Prof. Matteo Iannacone about Adaptive Immunity: 1ry & 2ry Lymphoid Organs. The Pdf explores the mechanisms of adaptive immunity, focusing on disease resistance and tolerance, and leukocyte extravasation, including 'ZIP codes' and topographic memory. This University Biology material is enriched with explanatory graphs.
See more19 Pages

Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Adaptive Immunity and Disease Mechanisms
Author: Onur Can Görmez Prof. Matteo Iannacone Basic Mechanisms of Diseases, MI3 07/11/2023 Adaptive Immunity: 1ry & 2ry Lymphoid Organs In general, defense strategies limit the virulence associated with the invading pathogens. They can be divided in different components. On one hand, we have resistance. Resistance limits the negative impact of infection on host fitness by reducing the pathogen burden. This is basically a function of the immune system, and this is what we're going to discuss during next lectures. The way you deal with a pathogen is by getting rid of them. This is how organisms are evolved in order to limit the negative impact on hosts. However, I would like to spend the first few minutes of this class by telling you about another mechanism, by which an organism can limit the impact of an infection on the host fitness. Host fitness is referred as disease tolerance. This is not the immunological tolerance, which we will talk about later, it is a concept that originated in plant biology field. It is how plants are dealing with infections. For instance, plants do not have an adaptive immune system. The way plants cope with infection is by decreasing the susceptibility to damage. Thus, instead of having any impact on the microorganism, disease tolerance comprises another mechanism that decrease the susceptibility to tissue damage or any other fitness costs.
Disease Trajectories
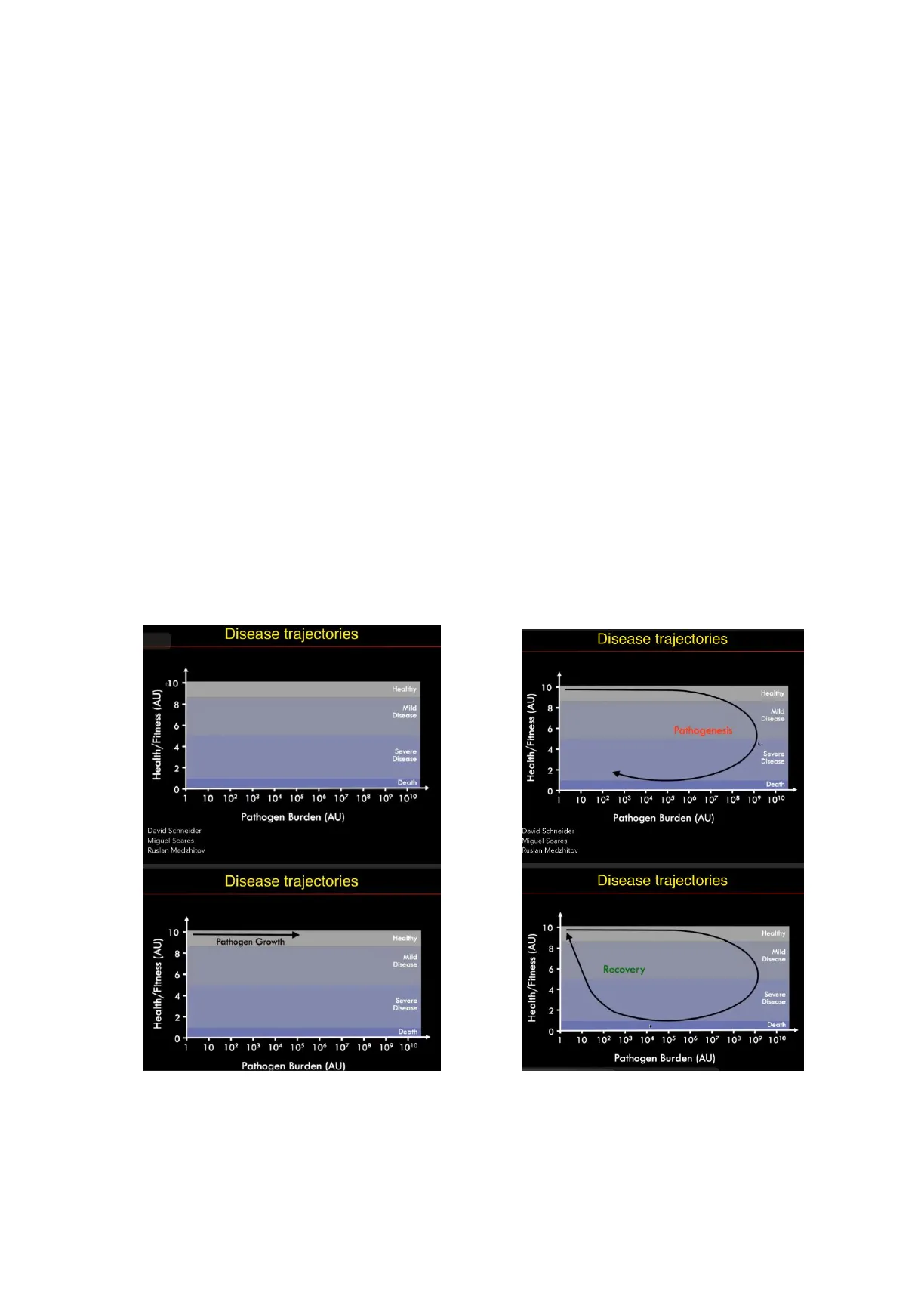
Disease trajectories Disease trajectories 10 Healthy Health/Fitness (AU) 8 Milo Disease 6 4 - Severe Disease 2 Death 0 0 - 1 10 102 103 104 105 106 107 108 109 1010 Pathogen Burden (AU) Pathogen Burden (AU) David Schneider Miguel Soares Ruslan Medzhitov Disease trajectories Disease trajectories 10 Healthy Health/Fitness (AU) 8 Mil 8 Milo Disease 6 - 4 Severe Disease 2 Death 0 0 + 1 10 102 103 104 105 106 107 108 10º 1010 1 10 102 103 104 105 106 107 108 10º 1010 Pathogen Burden (AU) Pathogen Burden (AU) Health/Fitness (AU) 8 Mild Disease 6 - Pathogenesis 4 Severe Disease 2 - Death 1 10 102 103 104 105 106 107 108 109 1010 David Schneider Miguel Soares Ruslan Medzhitov 10 Health/Fitness (AU) Pathogen Growth Healthy Disease 6 - Recovery 4 Severe Disease 2- Death 10 Healthy Page 1 of 19Author: Onur Can Görmez Prof. Matteo Iannacone Basic Mechanisms of Diseases, MI3 07/11/2023 Let's explain these concepts with these graphs. Health/fitness is in the Y axis. Let's say it is for 10- or 20-year-olds, who are healthy and happy. On the X axis we have the pathogen burden. If you have an infection, in the first few days, the pathogen breaches the barriers, such as skin or mucosa membranes, and it finds nutrients. Thus, it starts proliferating exponentially. This phase, which is characterized by this huge pathogen growth, does not have any impact on host fitness in the very beginning. The host remains healthy and happy. This is the classic incubation phase. For example, you went to a party, thus you had a superspreading event, and you got infected with SARS COV-2. For two or three days you felt nothing, but during this period SARS COV-2 is replicating in your upper and lower respiratory tract. Nevertheless, at some point, you do have this inflection of the curve. This is when the fitness of the host is decreasing. Thus, first, there is a mild disease that can progress to a severe one. Moreover, there is this inflection point where the curve turns to the left, this is when the immune system is kicking in and having an impact on pathogen growth. If you are at the upper portion of the curve, it is very different from when you are at the lower portion of the curve with the same pathogen burden. Basically, you can have a different impact of fitness with the same pathogen burden. Although these are still theoretical concepts, I think they can have potential for therapeutic consequences. This is because, these strategies that you might want to adopt when treating a patient, who has, for example, a pathogen burden of 10 to the power of 5 of any pathogen, are very different depending if you are in the upper portion of the curve or in the lower portion of the curve. In the upper portion of the curve, you probably want to have strategies that impact the pathogen burden, and you would like to give antivirals and antibiotics. Nevertheless, in the lower portion of the curve, the immune system is already kicking in, and the pathogen has already decreased. The immune system is working perfectly well, but here you want to increase host fitness, you do not need to reduce the pathogen anymore. In order to have complete recovery, you need to move vertically, thus you need to increase host fitness.
Disease Resistance vs Tolerance
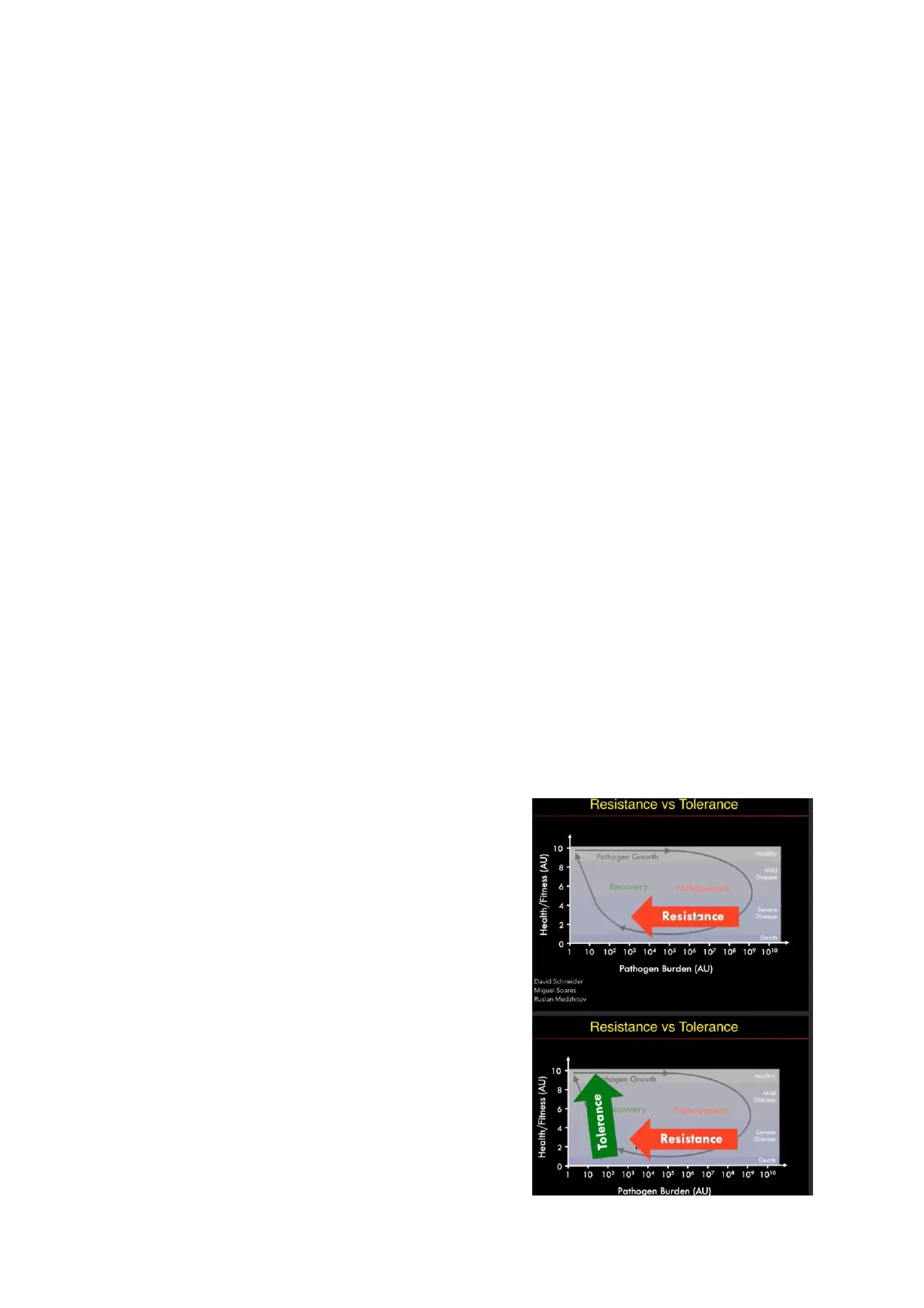
We refer to as a "resistance", any mechanism that can shift this curve to the left. This is the job of the immune system, and this is what we are going to talk about for the rest of the remaining five classes. We talk about "disease tolerance" for anything that shifts the curve up. Tolerance limits the negative impact of infection on host fitness, while decreasing the host susceptibility to tissue damage or any other fitness costs caused by the pathogen or by the immune system. At the point of 10^5, the host is sick not only because of the pathogen, but most likely because of immunopathological consequences like excessive inflammation and collateral tissue damage. When we talk about tolerance, even though it is a new concept, it is called "transcriptional stress and damage Resistance vs Tolerance 10 Healthy Health/Fitness (AU) 8 - Mild Disease 6- Recovery Pathogenesis 4 Severe Disease 2 0 1 10 102 103 104 105 106 107 108 109 1010 Pathogen Burden (AU) David Schneider Miguel Soares Ruslan Medzhitov Resistance vs Tolerance 10 Health/Fitness (AU) thogen Growth Healthy 8 Mild Disease 6 ecovery Pathogenesis 4 Resistance Severe Disease 2 Death O - 10 102 103 104 105 106 107 108 10º 1010 Pathogen Burden (AU) Page 2 of 19 Tolerance Resistance Death Pathogen GrowthAuthor: Onur Can Görmez Prof. Matteo Iannacone Basic Mechanisms of Diseases, MI3 07/11/2023 response network". For example, metabolic adaptation of tissues that renders them less susceptible to host damage. This is something plants and mammals do, and it refers to disease tolerance. I am not going to go into the details of this, but I just introduced the concept.
Smallpox and History of Adaptive Immunity
We are talking about adaptive immunity, and one of the key features of adaptive immunity is "memory". Memory, as a concept, has already been recognized many years ago, in particular in the western world. We have the first written evidence of it during the Peloponnesian War. Thucydides was reporting a disease, probably "yersinia pestis", bubonic plague hitting Athens during the 5th century BCE. What he was describing here was the immune memory. He was observing people who got sick by the bubonic plague but did not die.
Edward Jenner's First Immunological Experiment
Edward Jenner: First Immunological Experiment The beginning of adaptive immunity or experimental immunology traces back to Edward Jenner during the late 1700s, around INQUIRY THE CAUSES AND EFFECTS 1796, in England. Edward Jenner noticed that THE VARIOLE VACCIN.K. A DISEASE --- there was a disease similar to smallpox, THE COW FOX. which is called cowpox, and the people who - were handling and milking cows were Jenner: Smallpox is Stemmed. Painting by Robert Thom, Digital Image from The University of Michigan protected against smallpox. He hypothesized Rare Books and Special Collections Francis A. Countway Library of Medicine that there was something in cowpox, which was protective against smallpox. He took some material from people who had cowpox, which was a minor disease, and inoculated this to kids, including his oun kid. Two weeks later he then inoculated them with material coming from a smallpox lesion, which was highly lethal, and all the kids were protected. This is an experiment that would not go on with today's ethical committees, but at that time it did. We remember him as the first immunologist because all the kids were protected, but he was also extremely lucky. He did not know a lot of things that we now know. For instance, he could not know that this was caused by viruses and that in the skin lesions viruses are present. This means that, through a number of coincidences, he made this work. Basically, he prayed upon the practice, which took place centuries back in China. It was called "variolation". Variolation is intentional inoculation of an individual with smallpox material, and it traces back to 16th-century China. Smallpox had a mortality of 30%, which is huge, while variolation had mortality of 3%. It was a huge improvement, but still three out of a hundred kids that were variolated died. Variolation was directly using material from smallpox lesions. It was not exactly safe. Edward Jenner made an improvement by using cowpox lesions, and it was a great success.
Smallpox Eradication and Historical Impact
Page 3 of 19Author: Onur Can Görmez Prof. Matteo Iannacone Basic Mechanisms of Diseases, MI3 07/11/2023 Rulers killed by smallpox Smallpox Number of countries with one or more cases per month 15 smallpox officially eradicated C 1965 197 1975 1980 Year * King Ramses V of Egypt (pictured) * Queen Mary II of England * Emperor Joseph I of Austria * King Luis I of Spain * Tsar Peter II of Russia * Queen Ulrika Elenora of Sweden * King Louis XV of France Source: World Health Organization 1157 B.C. Estimated to have lead to 300 million deaths in the 20th century. During 20th century alone, it is estimated that 300 million people died because of smallpox. Number of 30 countries with one or more cases per month It was a huge health burden. Even very famous rulers died because of smallpox. It smallpox 15 officially eradicated took about 200 years to eradicate smallpox. The first experiment of Jenner was in 1796, and in 1979 WHO declared that the planet 1975 0 earth is free of smallpox. It is the only human 1965 1970 pathogen that has been eradicated so far. We are also very close to eradicating polio virus, but we are not there yet, there are still 10s of cases occurring in some countries like Afghanistan, Pakistan and some regions of Africa. Despite a massive effort and all the money put in, it is still not completely eradicated. Smallpox was eradicated thanks to a massive campaign made especially during 1950s and 60s. WHO organized these vaccination campaigns to reach every single person in remote corners of the world to immunize everybody. After 1976, for three years, there were no more cases of smallpox, and in 1979 WHO declared smallpox eradicated. It is not completely gone, but it is still in freezers in USA and Russia. Thus, there are labs in the world that have smallpox virus, but there was not a single case after 1976. It was arguably the biggest success in the history of medicine. Of course, not everybody was happy with the general vaccination. Starting from the early 1800s in England, there were some people that were scared and they claimed that the practices that Jenner was promoting were dangerous for people.
Contributions of Immunology
Immunology saved millions of lives, and trillions of dollars in agriculture. You can see a series of diseases that are almost completely gone thanks to vaccination. It is estimated that one third of all Nobel prizes in physiology or medicine are either awarded to immunology or had something to do with immunology. Page 4 of 19 Parham Figure 1.1 Figure 1.1 The Immune System, 4th ed. [C Garland Science 2015) Kills about 1/3 of those infected. Many who live are disfigured. 30
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
