Cervical cancer, uterine pathologies, and robotic hysterectomy
Slides from S. Padovano about cervical cancer. The Pdf, a university-level presentation, explores cervical cancer, uterine pathologies, and surgical techniques like robotic hysterectomy, including key anatomical structures and complication management.
See more21 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Hysterectomy and Anatomical Concepts
S. Padovano, V. Puglisi 1.04.2025 - OB/GYN - Prof. Costantini Cervical cancer During the last lesson, we talked about both endometrial and myometrial pathologies, including benign and malignant conditions. One of the most important surgical procedures for these types of cancers is the hysterectomy. So now, I'd like to apply some of the anatomical concepts we covered in the first lesson to explain how we perform a baseline hysterectomy. We're not discussing a radical hysterectomy here-that's typically used for cervical cancer. Instead, we're talking about a baseline hysterectomy, which is used for conditions like endometrial cancer, sarcomas, or even benign diseases. As you may remember, there are specific structures that help maintain the position of the uterus. One of these is the round ligament.
(the video is playing)
Robotic Hysterectomy Procedure
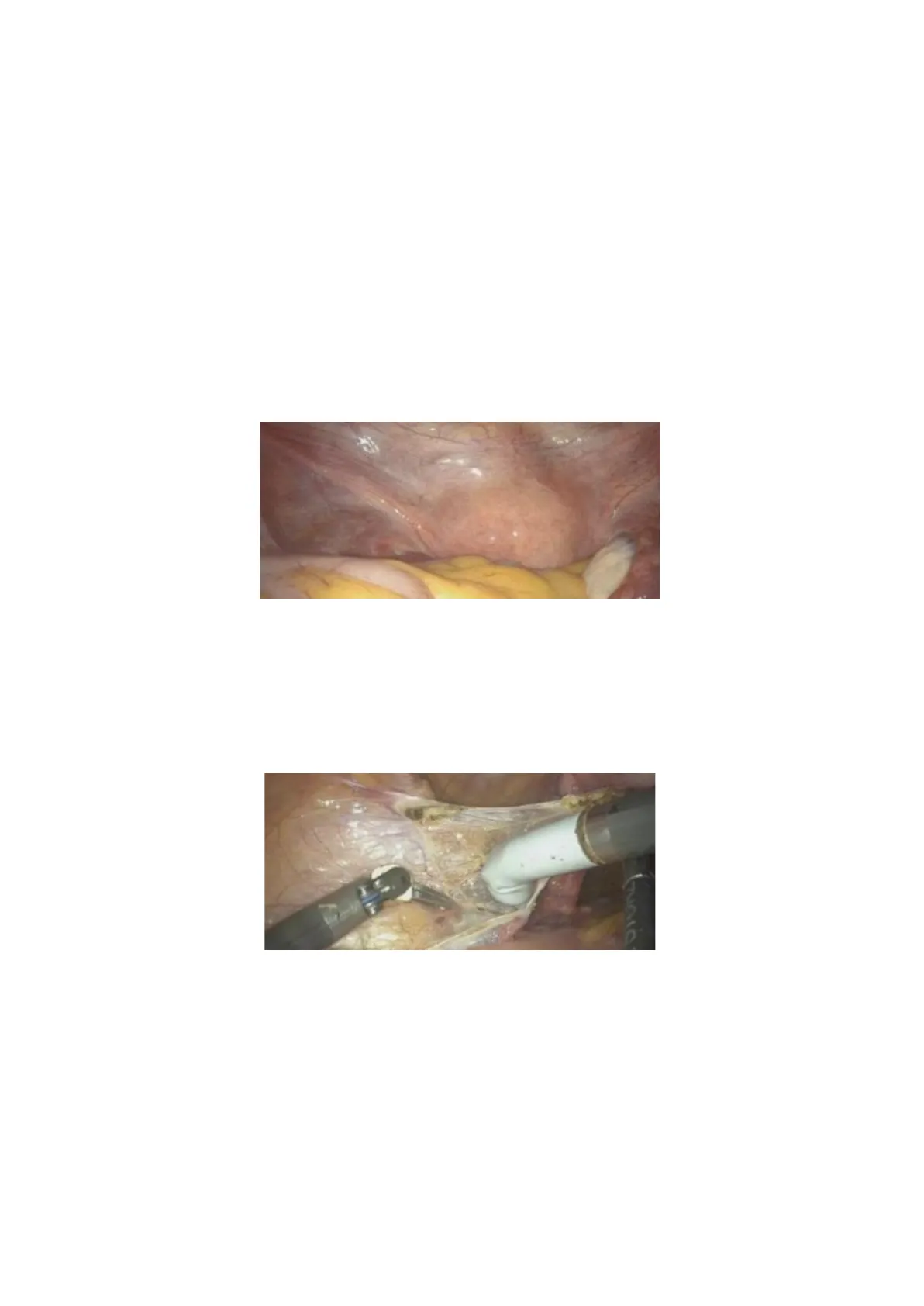
All the procedures we're discussing are performed using robotic surgery, and we use a uterine manipulator to help move the uterus during the operation. The first step is to cut the round ligament. Once it's cut, we gain access to the retroperitoneal space, where we can identify the key vascular structures that need to be either cut or preserved. Gunia One of the most important structures to identify is the ureter, that we must, of course, preserve. The next step is to locate, within the retroperitoneum, the vessels and the so-called "ureteric point," where we need to pay special attention. One crucial vessel to find is the umbilical artery.
Uterine Artery and Ureter Identification
As we mentioned, the uterine artery often branches off from the umbilical artery. While textbooks typically describe it as originating from the internal iliac artery, in practice, it often arises from the umbilical artery. Once we identify the umbilical artery, we can locate the ureter. If you remember, we said, "the water passes under the bridge." In this analogy, the "water" is the ureter, and the "bridge" is the uterine artery, which passes over it. Why is this important? If possible, we place a clip at the base of the uterine artery to stop the blood flow to theuterus, which helps reduce bleeding when we perform a total hysterectomy. We repeat the same steps on the opposite side.
Vessels and Ligament Dissection
The structure near the umbilical artery is the external iliac vessel. When performing a sentinel lymph node biopsy or lymphadenectomy, these vessels serve as important landmarks. After identifying all the structures, we create a window above the ureter to ensure we don't damage it when cutting the infundibulopelvic ligament.
- As a reminder, the uterine artery travels from lateral to medial and divides into two branches: one that supplies the body of the uterus and a smaller one that goes to the cervix. If we need to remove the uterus, we must cut this artery. In the case of benign disease or for endometrial cancer and sarcomas, we can cut the uterine artery at the level of the uterine body.
That's the uterine artery. We place the clip here, where the uterine artery arrives. Therefore, there is minimal bleeding, especially because we close the artery at its base before proceeding. After cutting the arteries, the next step is to prepare both the anterior and posterior planes. Anteriorly, we need to identify and mobilize the bladder. This structure here is the bladder, and we must create enough space to perform the colpotomy without causing any injury.
Bladder Mobilization and Colpotomy
To do this, we develop the vesico-uterine space by opening the peritoneum and carefully dissecting in this area. The incision is made through the peritoneum, and here you can see the bladder and the Foley catheter. Once this part is prepared, we identify the cervix and then the vagina.
Uterine Manipulator and Pneumoperitoneum
In this case, we're using a uterine manipulator, which includes valves to help guide the incision. Alternatively, a sponge can be placed inside the vagina to maintain the pneumoperitoneum and guide the colpotomy. If we don't place anything in the vagina, we risk losing the pneumoperitoneum when the vaginal wall is opened. We are demonstrating a robotic hysterectomy, but the steps are the same for laparoscopic and open abdominal (laparotomic) approaches. Using robotic assistance just makes it easier to visualize and explain the procedure.After cutting the round ligament and entering the retroperitoneal space, we continue the dissection around the cervix.
Uterosacral Ligaments and Vaginal Cuff Closure
These are the uterosacral ligaments, which are thick and strong, so we must coagulate them carefully. You can observe the tension they apply to the uterus. After completely detaching the uterus, we remove it through the vagina. The final step is to close the vaginal cuff. This procedure is one of the most fundamental surgeries in gynecology.
Cervical Diseases and Pathologies
After discussing pathologies involving the uterine body, we move on to cervical diseases, which affect a different anatomical compartment.
- Cervical pathologies can be benign or even physiological. One common example is cervical ectropion, often seen during a speculum exam, especially in multiparous women. This condition is normal and occurs when the endocervical columnar epithelium is exposed on the ectocervix. Because this tissue is thinner than the squamous epithelium, it is more prone to minor bleeding and irritation.
Benign Cervical Conditions
PHYSIOLOGY BENIGNE DISEASE vagina CERVICAL POLYP Nabothian cysts on the cervix ECTOPY - ECTROPION CONGENITAL MALFORMATION HYPERTROPHY CERVICITIS NABOTH CYST CERVICAL ENDOMETRIOSIS Other benign cervical conditions include congenital anomalies, like a septate uterus, which may be associated with a double cervix or even vaginal septa. It's important to thoroughly examine the cervix in these cases. Infections of the vagina may also spread to the cervix, especially those caused by Trichomonas or Chlamydia, leading to cervicitis. Rarely, cervical endometriosis can occur, presenting with lesions that have a characteristic color, often purplish or bluish, depending on the age and stage of the bleeding cycle. We previously discussed endometrial polyps, but polyps can also form in the cervix. These cervical polyps can often be seen protruding from the external os during a speculum exam. Sometimes, they become more noticeable during pregnancy due to hormonal changes that affect the cervical mucosa. Another common benign finding is the presence of Nabothian cysts. These appear as small, whitish cysts on the cervix. They are benign and not dangerous, but they can change the appearance of the cervix and are sometimes visible on ultrasound due to their characteristic internal structure.
HPV and Cervical Cancer
- In addition to benign conditions, the cervix can also be affected by pre-invasive and invasive diseases, most of which are caused by a single pathogen: HPV (Human Papillomavirus). HPV is responsible for both precancerous and cancerous cervical lesions. More than 90% of cervical cancers are associated with HPV infection.
However, not all HPV infections lead to cancer. There are over 150 types of HPV, but only about 20 of them are considered high-risk for cervical cancer. Some HPV types are low-risk and cause benign lesions, while others are linked to cancer development. We know that HPV (Human Papillomavirus) is one of the most common sexually transmitted infections, particularly affecting younger populations. In fact, by the age of 19, more than 50% of women have already been exposed to the virus. The distribution of HPV-related cancers varies by age and geographical region.
Global Burden of HPV-Attributable Cancers
A 250000 Cervix uteri carcinoma This difference is mainly Other anogenital cancer Global burden of cancer attributable to infections in 2018: Head and neck cancer a worldwide incidence analysis due to the availability of 200000 Catherine de Martel Damien Georges, Freddie Bray, Jacques Ferlay, Gary M Clifford oa preventive measures such 150000 HPV-attributable cancers (of which 80% are cervical)-> inverse association between age-standardised incidence rates (ASIR) and 100000 income level, increasing from 6.9 cases per 100.000 person/yrs in high-income vs and 9.2 in upper-middle to in lower-middle-income 0000- vs 16.1 in low-income countries. as vaccination and screening programs. In areas where access to these This trend is mainly driven by access to cervical screening for detection of precancerous lesions, which has resulted in substantial 250000- HPV 16/18 HPV 6/11/31/33/45/52/58 decreases in incidence and mortality in high-income settings but is Other HPV types often unavailable in low-income and lower-middle-income countries resources is limited, cervical cancer is more 200 000 prevalent. HPV-related cancers are the second 150 000 most common cancers 100 000 Age-standardised mortality rate 50000 (per 100 000women-years) caused by a virus. While 2.5 to <5.6 Number of cancer cases attributable to HPV Number of cancer cases attributable to HPV 8.8 to <16.8 5.6 to <8.8 cervical cancer is the most 0- Men Women Women Men Upper-middle income Men Women Nen 2.5 16.8 in <64.3 well-known HPV-related Low income Low-middle income Women High income cancer, the virus can also cause other genital cancers, such as vulvar and vaginal cancer, as well as anal, penile, and even some head and neck (oropharyngeal) cancers. The type of cancer depends on how the virus spreads and which areas of the body it infects. There are many types of HPV, but only a small portion of infections lead to cancer. Most HPV infections clear up on their own - about 80% of them within one to two years. Only persistent infections carry the risk of progressing into precancerous lesions, and even then, many of these lesions also regress spontaneously. However, some low-grade lesions can progress to high-grade precancerous lesions over time. If not treated, these high-grade lesions can eventually develop into cervical cancer. This progression typically occurs over many years - often 10 years or more - which gives us time to monitor, detect, and treat precancerous changes before they become malignant.
HPV Types and Cancer Risk
- HPV types are generally divided into low-risk and high-risk categories. Low-risk types can cause benign conditions such as genital warts. If we observe warts in the vaginal or vulvar area, we should test for HPV, as the patient may carry both low-risk and high-risk types simultaneously. High-risk HPV types are those most commonly associated with cancer, with types 16 and 18 being responsible for the majority of cervical cancer cases.
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
