Immunodeficienze primarie: sindrome di Wiskott-Aldrich e artrite idiopatica
Documento dall'Università sulle immunodeficienze primarie. Il Pdf esplora la sindrome di Wiskott-Aldrich e l'artrite idiopatica giovanile, con fenotipi clinici, diagnosi e trattamenti. Questi appunti di Biologia per l'Università, prodotti nel 2023, offrono una panoramica chiara e dettagliata sugli argomenti trattati.
Mostra di più36 pagine

Visualizza gratis il Pdf completo
Registrati per accedere all’intero documento e trasformarlo con l’AI.
Anteprima
Sbobinatore e Revisione
Sbobinatore: Alberto Cucco Revisionatrice: Maria Eugenia Gargiulo Prof. Merli 10/03/2025(16:30-18:30)
Immunodeficienza Primaria
Last lesson we talked about the inborn errors of immunity, today we will continue with some of the most important ones. They are not the most frequent, but the most famous and most typical of the pediatric age:
- CLASSICAL WISKOTT-ALDRICH SYNDROME
- ISOLATED X-LINKED THROMBOCYTOPENIA
- INTERMITTENT X-LINKED THROMBOCYTOPENIA
- ISOLATED X-LINKED NEUTROPENIA
- X-LINKED MYELODYSPLASIA
Sindrome di Wiskott-Aldrich (WAS)
Sindrome di Wiskott-Aldrich: Fenotipo Clinico
- males
- thrombocytopenia with small PLT vol
- muco-cutaneous bleedings
- bloody diarrhea
- CNS hemorrhages
- eczema
- progressive immunodeficiency
The first disorder we will discuss today is Wiskott-Aldrich Syndrome (WAS): a primary immune deficiency categorized as an inborn error of immunity. This condition is associated with thrombocytopenia, making it relatively easy to identify. If a young male patient presents with thrombocytopenia, recurrent infections, and eczema, WAS should be considered as a potential diagnosis. Since WAS is an X-linked disorder it exclusively affects males. Regarding bleeding, we can have mucocutaneous 1:150.000 male newborns bleeding, bloody diarrhea and also hemorrhages of the central nervous system. Given a male patient with thrombocytopenia, eczema, and a history of infections, these symptoms alone should raise suspicion for WAS. However, it is important to note that this is a rare disease, with an incidence of approximately 1 in 150,000 live births. In Italy, where annual births are currently below 500,000, this translates to approximately one to two affected male infants per year.
Fenotipi WAS / XLT: Test di Conferma
+ Mutation analysis of WASP gene and + analysis of expression of the WAS protein
Test di Conferma WAS / XLT
+ Mutation analysis of WASP gene and + analysis of expression of the WAS protein
Classificazione Clinica (Zhu et al.)
| Disease | XLT | WAS | |||
| Score | 1 | 2 | 3 | 4 | 5 |
| Thrombocytopenia | + | + | + | + | + |
| Low PLT count | + | + | + | + | + |
| eczema | - | (+) | + | ++ | +/++ |
| Immunodeficiency | -/(+) | (+) | + | + | |
| Infections | - | (+) | + | +/++ | +1++ |
| Autoimmunity and/or tumors | - | + |
Indeed, WAS is not a single disease, but a spectrum of different diseases due to possible variable expression of the protein of the mutated gene. This disease can present itself in different way: we can have a classical Wiskott-Aldrich phenotype (the one presented in the previous slide), but we can have just an isolated thrombocytopenia without other features. The thrombocytopenia can be also intermittent, not continuous, or we can have isolated neutropenia or myelodysplasia. The mutated protein, which is the WASP protein, is a protein that is fundamental for the cytoskeleton, and thus the variable phenotype. The classical phenotype of WAS is not the only manifestation of mutations in the WASP gene.Sbobinatore: Alberto Cucco Revisionatrice: Maria Eugenia Gargiulo Prof. Merli 10/03/2025(16:30-18:30)
Altre Presentazioni Cliniche
Other clinical presentations include:
- Isolated thrombocytopenia (X-linked thrombocytopenia, XLT)
- Intermittent X-linked thrombocytopenia
- Neutropenia
- Nail dysplasia
Thus, the clinical phenotype varies depending on the type of mutation.
Diagnosi
Dr. Zhu has developed a clinical score based on some features of the disease, including: thrombocytopenia, eczema, immune deficiencies, infection, and autoimmunity or tumors. Remember this concept is very important: every immune deficiency could predispose not only to infection, but also to autoimmunity and tumors. So, if you have only thrombocytopenia with low platelet volume, you will have an XLT, extreme thrombocytopenia. While, if you start to develop eczema, immune deficiency, infection, or autoimmunity, you will have a diagnosis of WASP. Looking at Doctor Zhu's score is important to understand the best treatment choice for the patient. You don't just have to analyze the mutation of WASP, but also the extraction of the protein through western blot or also intracytoplasmic staining through flow cytometry.
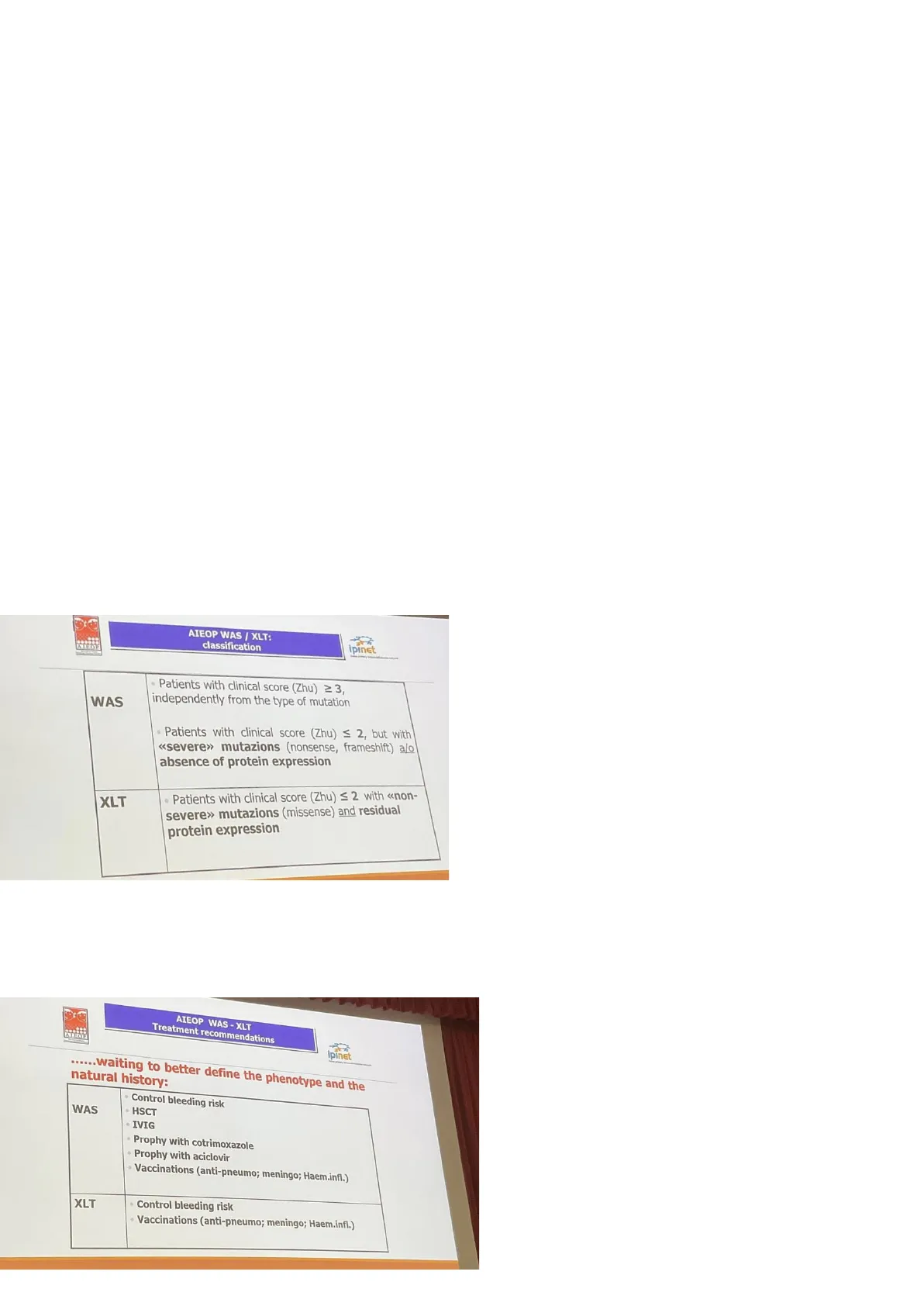
Classificazione AIEOP WAS / XLT
ATEST AIEOP WAS / XLT: classification ipinEt
WAS
- Patients with clinical score (Zhu) ≥3, independently from the type of mutation
- Patients with clinical score (Zhu) ≤ 2, but with «severe» mutazions (nonsense, frameshift) a/o absence of protein expression
XLT
- Patients with clinical score (Zhu) ≤ 2 with «non- severe» mutazions (missense) and residual protein expression
AIEOP (Associazione Italiana Ematologia Oncologia Pediatrica) and IPINET (Italian Primary Immune Deficiencies Network), propose this type of classification:
- You can have WASP in case of
- A clinical score equal or above 3
- A clinical score equal or below 2 with some mutations like non-self mutation, friendship mutation, and or absence of protein expression. These 2 will be classified as Wieschott-Aldrich syndrome.
- Clinical score less than 2 with no mutations can be classified as XLT.
This is important for treatment, because for WASP the treatment is hematopoietic stem cell transplantation, instead for XLT there's no indication of stem cell transplantation, this is important also for medical legal issues.
Raccomandazioni di Trattamento AIEOP WAS - XLT
ipinet ...... waiting to better define the phenotype and the natural history:
WAS
- Control bleeding risk
- HSCT
- IVIG
- Prophy with cotrimoxazole
- Prophy with aciclovir
- Vaccinations (anti-pneumo; meningo; Haem.infl.)
XLT
Control bleeding risk
- Vaccinations (anti-pneumo; meningo; Haem.infl.)
Raccomandazioni di Trattamento AIEOP WAS-XLT
-You need to control bleeding risk. Remember that you can transfuse these patients, because this is not an immune-mediated destruction. - You have to supplement immune globulins. - You have to perform a prophylaxis with cotrimoxazole for pneumocystis. - You have to give acyclovir.Sbobinatore: Alberto Cucco Revisionatrice: Maria Eugenia Gargiulo Prof. Merli 10/03/2025(16:30-18:30) - You also have to vaccinate patients. So, immune deficiencies can be vaccinated, but it depends on the type of immune deficiency.
Sindrome di Wiskott-Aldrich (WAS): Genotipo come Biomarcatore Predittivo per la Gravità della Malattia
WAS, a disease with a large variation in disease severity Mild WAS/XLT -+ classic WAS (disease progression possible) (KLT, X-linked thrombocytopenia) WAS variants dess Overall survival is better and disease-related events occur later in patients with class I variants
- Retrospective survey of 577 WAS patients
- Grouped by WAS variant:
- class l: missense variants in exon 1 or 2 + intronic variant c.559+5G>A
- class Il: all other variants
Conclusions: The type of genetic variant is a predictive biomarker for disease severity and survival in WAS. Patients with less severe variants experience a later onset of disease-related complications but remain prone to morbidity and premature mortality.
@ blood Visual Abstract
Last year, a study group performed a new type of analysis on this disorder: showing that certain variants like missense mutations in exon 1 or 2 or intronic variants have a bad prognosis. The others, instead, have a better prognosis. In this survival curve, the patients were censored at stem cell transplantation or gene therapy. What does censor mean? If the patient underwent stem cell transplantation or gene therapy, the follow-up stopped and the patient was not counted after that.
Malattia di Bruton e Disturbi Correlati: Agammaglobulinemia di Bruton (Agammaglobulinemia X-Linked)
Deficienza BTK / XLA: Periferia
γδ Yo pro T CD8 HSC LSC αβ CD4 Thymus BM JBTK pro B - X-linked Agammagl. - Autosomal recessive agammagl.
PERIPHERY γδ YO pro T CD8 HSC LSC αβ CD4 Thymus BM 1 LBTK O pro B % lymphocytes B ≤ 2; H, Iga, 15, BLNK Vallée et al. DOI: 10.1182/blood.2023021411
This disease is characterized by a mutation in the Bruton tyrosine kinase, which is a kinase that works after the PRO-B status of B-lymphocytes. This mutation leads to lack of mature B-lymphocytes and consequent hypogammaglobulinemia. In BTK deficiency T-cells are not affected and Pro-B Cells are in the bone marrow. This is a X-linked agammaglobulinemia and there are other types of autosomal recessive agammaglobulinemia, which are even rarer than X Linked agammaglobulinemia.Sbobinatore: Alberto Cucco Revisionatrice: Maria Eugenia Gargiulo Prof. Merli 10/03/2025(16:30-18:30)
Diagnosi con Citometria a Flusso
You can easily perform a diagnosis with flow cytometry showing B lymphocyte frequency below 2%. Perform:
- CBC
- serum IG levels
- B cell subset . Check antibodies for tetanus and hepatitis to easily diagnose this kind of disease.
Basically, some of these disorders are not so difficult to be diagnosed, apart from the molecular diagnosis which always confirms your diagnosis. With very few tests that are available everywhere, you can perform a brilliant diagnosis of a very rare disorder.
Difetti Primari dell'Immunità Umorale (Agamma; CVID)
- Onset after 6-12 months of age
- Upper and lower respiratory tract infections (otitis,sinusitis, bronchitis, pneumonia)
Agammaglobulinemia X-Linked (XLA)
- Prototype model of humoral primary immune-deficiency.
- Incidence 1:100.000 newborns.
- Genetic defect: BTK gene mutations
- Only males are affected: v Low/undetectable Ig serum levels Undetectable B cells in peripheral blood / Normal T and NK cell function.
Immunità Umorale Primaria
The problems of humoral immunity are shown after six months of age, because the baby loses the immunoglobulins from the mother.
Caratteristiche Cliniche
- Upper and lower respiratory tract infections which are obviously the most frequent infection of children.
- Otitis
- Sinusitis
- Bronchitis
- Pneumonia
- Bronchiectasis mainly due to bacteria.
Bruton was a soldier of the U.S. Army working at Walter Reed Hospital: from his name, the eponym of the disease.
Epidemiologia
The incidence is very rare: more or less ciao 2 or 3 cases per year in Italy. The gene affected is BTK coding for Bruton tyrosine kinase. Only males are affected: These are the diagnostic criteria, which is a repetition of previous slides. Remember, when a patient presents recurrent bacterial infection and early onset, think about that.
Criteri Diagnostici per XLA
Risultati Immunologici
- Absent low Ig serum levels
- Absent B cells
Risultati Clinici
- males
- Early onset
Bacterial infections
Conferma Molecolare
- BTK gene
Non hai trovato quello che cercavi?
Esplora altri argomenti nella Algor library o crea direttamente i tuoi materiali con l’AI.
