Definizione di embolia polmonare e tromboembolismo venoso
Slide del Prof. Nicola Ciavarella su Definizione Embolia Polmonare. Il Pdf, utile per studenti universitari di Biologia, illustra l'embolia polmonare e il tromboembolismo venoso, includendo epidemiologia, punteggio di Ginevra e cause di incremento del D-dimero.
Mostra di più53 pagine

Visualizza gratis il Pdf completo
Registrati per accedere all’intero documento e trasformarlo con l’AI.
Anteprima
DEFINIZIONE EMBOLIA POLMONARE
Occlusione acuta o cronica di un vaso arterioso polmonare
TROMBOEMBOLISMO VENOSO
Embolia polmonare e/o trombosi venosa profonda Terza causa di sindromi cardiovascolari acute dopo SCA e stroke
EPIDEMIOLOGIA
Incidenza EP e TVP
EP incidenza 39-115/100.000 ab/anno TVP incidenza 53-162/100.000 ab/anno
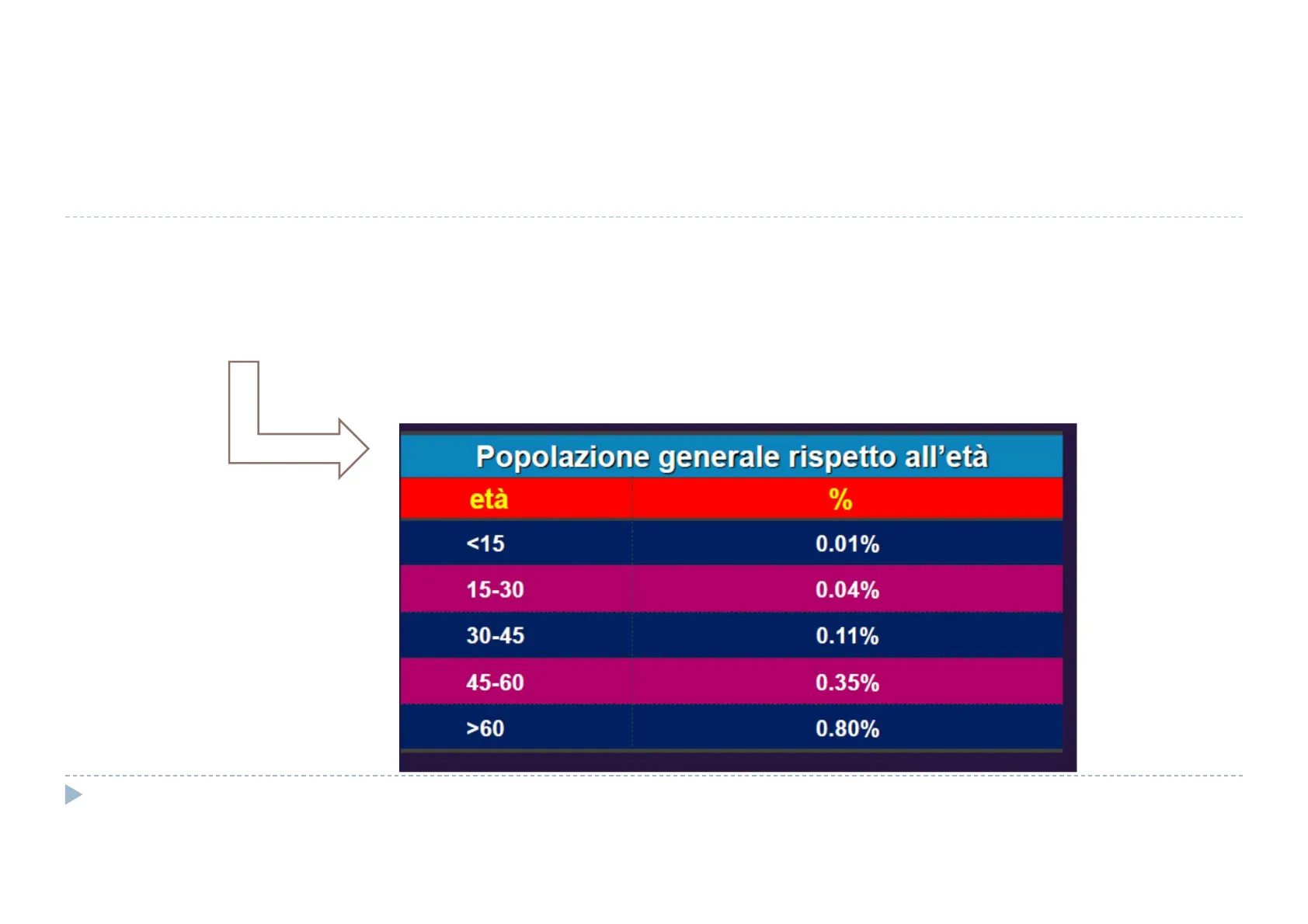
Popolazione generale rispetto all'età
età % <15 0.01% 15-30 0.04% 30-45 0.11% 45-60 0.35% >60 0.80%
EPIDEMIOLOGIA E GENERE
There is a complex relationship between the incidence of VTE and sex, as it is modified by age. Women have higher rates of VTE than men in those aged <55 years,50 which cor- responds to being premenopausal and the effect of estrogen as a risk factor for VTE. Men have higher incidence of VTE among those aged 60 to 80 years, and then among those aged 80+ years, women again have a higher incidence than men.1,50 The explanation for the observed increased rate among wom- en aged 80+ years is attributed to the longer life expectancy of women.50 Circ Res. 2016;118:1340-1347. DOI: 10.1161/CIRCRESAHA.115.306841.)
MORTALITA'
Table. Incidence, Mortality, YLD, and DALY Estimates of Thrombotic Conditions per 100 000 Population Measure Ischemic Heart Disease* Ischemic Stroke* Atrial Fibrillation* Venous Thromboembolism Incidence 1518.7 (2013) 114.3 (2013) 77.5 males (2010), 59.5 females (2010) 115-269 (2010)1 Mortality 105.5 (2010) 42.3 (2010) 1.7 (2010) 9.4-32.3 (1998-2008)15,16 YLDS 5.8 (2013) 2.7 (2013) 0.9 (2013) Not available DALY 654-2855 (2010)17 217-1361 (2010)18 45.9-64.5 (2010) Not availablet DALY indicates disability-adjusted life-year; and YLD, years lived with disability. *Estimates from the Global Burden of Disease project.3,11,12 tA single study estimated hospital-associated DALYs of pulmonary embolism to be 7.6.19 Circ Res. 2016;118:1340-1347. DOI: 10.1161/CIRCRESAHA.115.306841.)
Fattori di rischio
La triade di Virchow
- ipercoagulabilità
- stasi
- danno endoteliale Virchow. Cellular Pathology as based upon phisyological and pathohistology. 7th American ed. Chance, DeWitt, trans. New York: 1860; 236
FATTORI PREDISPONENTI
Fattori di rischio forti
Paziente versus ambiente Transitori versus permanenti Strong risk factors (OR > 10) Fracture of lower limb Hospitalization for heart failure or atrial fibrillation/flutter (within previous 3 months) Hip or knee replacement Major trauma Myocardial infarction (within previous 3 months) Previous VTE Spinal cord injury ESC Guidelines
Fattori di rischio moderati
Paziente versus ambiente Transitori versus permanenti Moderate risk factors (OR 2-9) Arthroscopic knee surgery Autoimmune diseases Blood transfusion Central venous lines Intravenous catheters and leads Chemotherapy Congestive heart failure or respiratory failure Erythropoiesis-stimulating agents Hormone replacement therapy (depends on formulation) In vitro fertilization Oral contraceptive therapy Post-partum period Infection (specifically pneumonia, urinary tract infection, and HIV) Inflammatory bowel disease Cancer (highest risk in metastatic disease) Paralytic stroke Superficial vein thrombosis Thrombophilia ESC Guidelines
Fattori di rischio deboli
Paziente versus ambiente Transitori versus permanenti Weak risk factors (OR < 2) Bed rest >3 days Diabetes mellitus Arterial hypertension Immobility due to sitting (e.g. prolonged car or air travel) Increasing age Laparoscopic surgery (e.g. cholecystectomy) Obesity Pregnancy Varicose veins ESC Guidelines
FATTORI PREDISPONENTI TROMBOFILIA
Prevalenza e rischio di trombosi
Guidance for the evaluation and treatment of hereditary and acquired thrombophilia 157 Table 2 Prevalence and thrombosis risk for selected thrombophilias Thrombophilia Prevalence Relative (absolute annualized) risk of risk of Initial VTE* Relative Relative (absolute annualized) risk of initial VTE, OCP users". Relative (absolute annualized) risk of initial VTE, HRT users be Relative (absolute) risk of initial VTE, pregnancy" Fattore V Leiden FVL 2-7 % 3.48-5.51 1.1-1.8 2.47-15.04 1.4-13.16 (1.6-5.97 %) 8.3 Heterozygous (0.05-0.2 %) (0.1-0.6 %) (0.8-4.6 %) FVL 0.06-0.25 % 6.79-19.29 1.8 Uncertain Uncertain 34.4 Homozygous (0.8 %) PGM 1-2 % 2.25-3.48 0.7-2.3 3.60-8.63 (2.85 %) 6.8 Heterozygous (0.13 %) (0.3-5.6 %) PGM Rare 2.19-20.72 Uncertain Uncertain Uncertain 26 Homozygous 0.1 % 1.13-5.04 2.7 3.79-76.47 Uncertain (4 %) FVL & PGM Heterozygosity (0.42 %) (0.17 %) Deficit prot. C e prot. S PC deficiency 0.2-0.5 % 10 1.8 1.7-23.9 (2.96 %) 4.8 (0.4-2.3 %) (1.7-7.1 %) (0.4-8.9 %) PS deficiency 0.1-0.7 % 9.6 1.0 1.4-17.1 (2.3 %) 3.2 Deficit AT AT deficiency 0.02 % 10-30 2.6 1.4-115.8 (5.73 %) 4.7 (1.2-4.4 %) (2.5-5.1 %) (0.08-15.8 %) APS 2 % 7 1.5-6.8 0.3-3.1 (1.05-2.63 %) 15.8 Ab antifosfolipidi OCP oral contraceptive pill (containing estrogen), HRT hormone replacement therapy (containing estrogen), VTE venous thromboembolism, FVL factor V Leiden, PGM prothrombin Gene G20210A, PC protein C, PS protein S, AT antithrombin, APS antiphospholipid syndrome J Thromb Thrombolysis (2016) 41:154-164 DOI 10.1007/s11239-015-1316-1 (0.2-14.7 %) (0.7-3.2 %) (1.3-2.4 %) (1.4-25.8 %) Mutazione gene protrombina (0.2-78.3 %) Compound recurrent VTE
Valutazione della trombofilia
Question Guidance statement Timing of thrombophilia assessment When thrombophilia testing is performed, at what point in the patient's care should this be done? Do not perform thrombophilia testing at the time of VTE diagnosis or during the initial 3-month course of anticoagulant therapy. When testing for thrombophilias following VTE, use either a 2-stage testing approach (see text) or perform testing after a minimum of 3 months of anticoagulant therapy has been completed, and anticoagulants have been held. Remark Pregnancy, sex and estrogen use reduce the levels of Protein S. Use of sex specific reference intervals, and testing prior to pregnancy or while not receiving estrogen preparations is preferred. J Thromb Thrombolysis (2016) 41:154-164 DOI 10.1007/s11239-015-1316-1
FATTORI PREDISPONENTI
40% PAZIENTI NESSUN FATTORE PREDISPONENTE
FISIOPATOLOGIA
Increased RV afterloadª RV dilatation TV insufficiency RV O2 delivery RV wall tension Coronary perfusion of RV Neurohormonal activation Systemic BP Obstructive shock Myocardial inflammation Death CO RV O2 demand LV preload Intrapulmonary A-V shunting RV output RV ischaemia, hypoxic injury RV contractility DESC 2019 Figure 2 Key factors contributing to haemodynamic collapse and death in acute pulmonary embolism (modified from Konstantinides et al65 with permis- sion). A-V= arterio-venous; BP =blood pressure; CO = cardiac output; LV - left ventricular; O2 = oxygen; RV = right ventricular; TV = tricuspid valve. "The exact sequence of events following the increase in RV afterload is not fully understood.
PRESENTAZIONE CLINICA EP
Segni e sintomi non specifici !! Dispnea Dolore toracico Emottisi Presincope 0 Sincope 0 Asintomaticità
PRESENTAZIONE CLINICA EP
Instabilità emodinamica
Table 4 Definition of haemodynamic instability, which delineates acute high-risk pulmonary embolism (one of the following clinical manifestations at presentation) (1) Cardiac arrest Need for cardiopulmonary resuscitation (2) Obstructive shock68-70 (3) Persistent hypotension Systolic BP < 90 mmHg or vasopressors required to achieve a BP ≥90 mmHg despite adequate filling status Systolic BP < 90 mmHg or systolic BP drop ≥40 mmHg, lasting longer than 15 min and not caused by new-onset arrhythmia, hypovolaemia, or sepsis And End-organ hypoperfusion (altered mental status; cold, clammy skin; oliguria/anuria; increased serum lactate) BP= blood pressure.
PRESENTAZIONE CLINICA TVP
Dolore spontaneo o provocato Arrossamento locale 0 Calor 0 Tumor/edema franco Iperestesia cutanea Dolore alla dorsiflessione del piede (Homans) 0 Segno di Bauer
ESAMI DI LABORATORIO EP
DIpossiemia (60% pz ... ) O Ipocapnia 7 Alterazioni ECG Inversione onde T V1-V4 QR in V1 S1Q3T3 BBDx completo o incompleto Tachicardia sinusale Aritmie atriali Radiografia del torace
VALUTAZIONE DELLA PROBABILITA' DI EMBOLIA POLMONARE
Valutazione clinica + dati strumentali + fattori predisponenti
SCORE DI WELLS
Caratteristiche cliniche Score Segni e sintomi clinici di TVP (minimo di gonfiore alla gamba e dolorabilità alla palpazione delle vene profonde) 3 Diagnosi alternativa meno probabile della diagnosi di EP 3 Pulsazioni > 100 battiti/min 1.5 Immobilizzazione per un periodo > 3 giorni o intervento chirurgico nelle 4 settimane precedenti 1.5 Pregresso episodio di TVP o di EP 1.5 Emottisi 1 Neoplasia maligna (terapia in corso o negli ultimi 6 mesi o cure palliative) 1 Score totale > 4: EP probabile Score totale ≤ 4: EP improbabile
GENEVA SCORE
Items Clinical decision rule points Original version91 Simplified version37 Previous PE or DVT 3 1 Heart rate 75-94 b.p.m. 3 1 ≥95 b.p.m. 5 2 Surgery or fracture within the 2 1 past month Haemoptysis 2 1 Active cancer 2 1 Unilateral lower-limb pain 3 1 Pain on lower-limb deep venous 4 1 palpation and unilateral oedema Age >65 years 1 1 Clinical probability Three-level score Low 0-3 0-1 Intermediate 4-10 2-4 High ≥11 >5 Two-level score PE-unlikely 0-5 0-2 PE-likely >6 >3 b.p.m. = beats per minute; DVT = deep vein thrombosis; PE = pulmonary embolism.
D-DIMERO
Caratteristiche del D-Dimero
Prodotto di degradazione della fibrina Dosaggio plasmatico: Elevata sensibilità (>90%) Bassa specificità (10-40%) Elevato valore predittivo negativo Serve per ESCLUDERE EP/TVP ma non per confermare 0 Possibili falsi negativi: Cut off errato Durata dei sintomi Terapia anticoagulante in corso
CAUSE DI INCREMENTO DEL D-DIMERO
- Età avanzata
- Periodo neonatale
- Gravidanza fisiologica e patologica (incluso il puerperio)
- Pazienti ospedalizzati
- Pazienti con disabilità funzionale
- Infezioni (in particolare sepsi da Gram negativi)
- Neoplasie
- Interventi chirurgici
- Traumi
- Ustioni
- CID
- Tromboembolia venosa
- Cardiopatia ischemica
- Stroke
- Arteriopatia periferica
- Aneurismi
- Scompenso cardiaco congestizio
- Crisi emolitiche anemia falciforme
- Malattie infiammatorie intestinali
- Emorragie subaracnoidee ed ematomi sottodurali
- Altre emorragie
- ARDS
- Malattie epatiche
- Malattie renali
- Malattie infiammatorie croniche (es. LES, artrite reumatoide)
- Terapia trombolitica Prof. Nicola Ciavarella (coord.T.T.T. - HTA -A.Re.S. Puglia)
Non hai trovato quello che cercavi?
Esplora altri argomenti nella Algor library o crea direttamente i tuoi materiali con l’AI.
