Inquadramento e trattamento della pubertà precoce, Presentazione
Slide dall'Azienda Ospedaliero-universitaria Sant'Andrea su inquadramento e trattamento della pubertà precoce. Il Pdf esplora le manifestazioni fisiologiche e le cause, le nuove prospettive terapeutiche e l'impatto del COVID-19, utile per Biologia a livello universitario.
Mostra di più23 pagine


Visualizza gratis il Pdf completo
Registrati per accedere all’intero documento e trasformarlo con l’AI.
Anteprima
Inquadramento della pubertà
Inquadramento e trattamento della
pubertà precoce
Alessandro Ferretti
SISTEMA SANITARIO REGIONALE
AZIENDA OSPEDALIERO-UNIVERSITARIA
SANT'ANDREA
SAPIENZA
UNIVERSITÀ DI ROMA
STVDI
VRBISPUBERTA'
Periodo della vita
caratterizzato dalla comparsa
e dalla progressione dei
caratteri sessuali secondari
fino al raggiungimento della
capacità riproduttiva
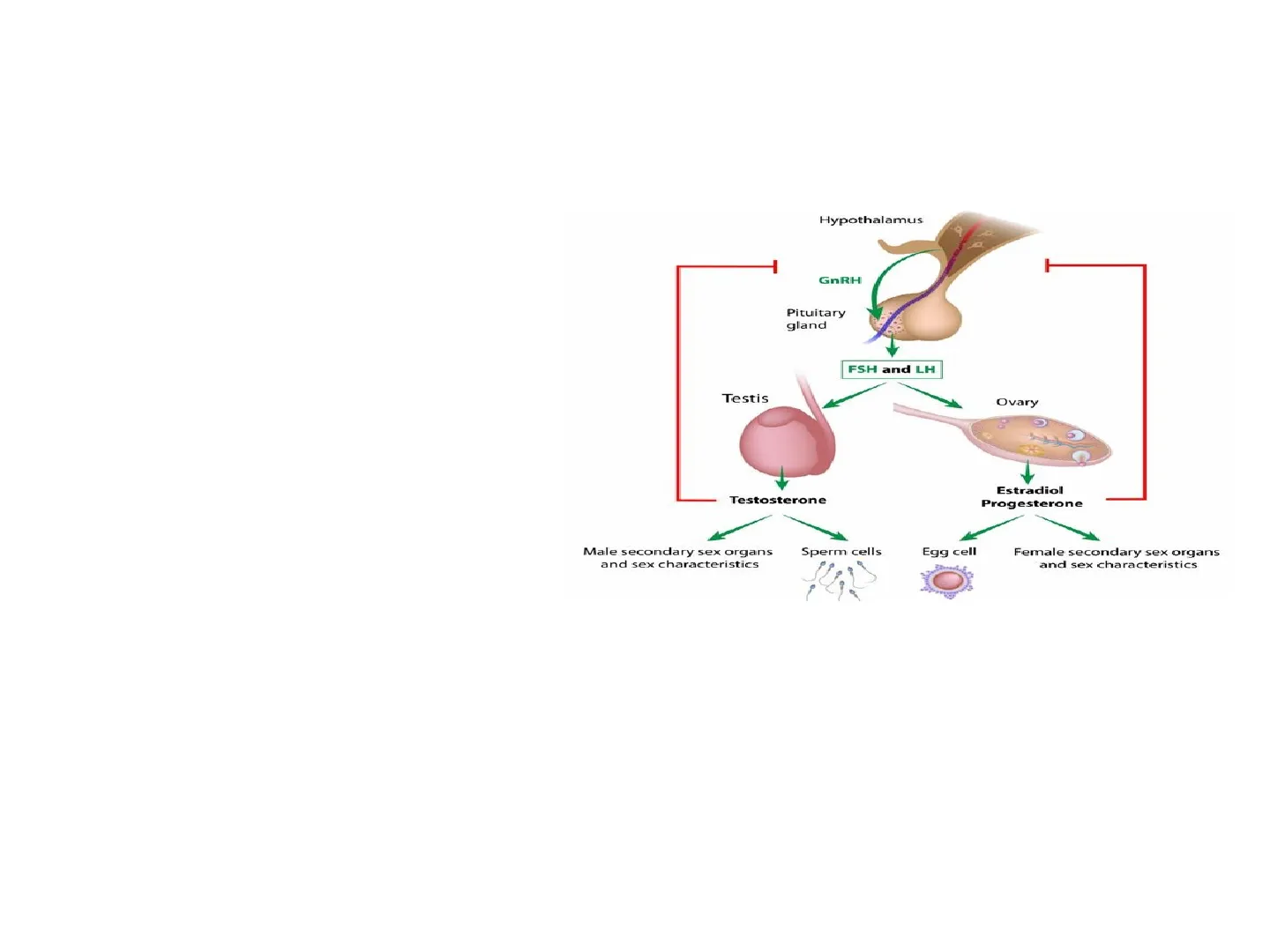
Hypothalamus
GnRH
Pituitary
gland
FSH and LH
Testis
Ovary
O
Testosterone
Estradiol
Progesterone
Male secondary sex organs
and sex characteristics
Sperm cells
Egg cell
Female secondary sex organs
and sex characteristics
Si manifesta fisiologicamente (±2DS):
-tra 8 e 13 anni nelle femmine
-Tra 9 e 14 anni nei maschi
L'attivazione puberale è il risultato di una complessa interazione dinamica tra
fattori genetici, nutrizionali, ambientali ed epigeneticiPUBERTA'
Stadi di Tanner
Breast
Stage 1
Stage 2
Stage 3
Stage &
Stage S
Pubic hair Stage 1
Stage 2
Stage 3
Stage 4
Stage 5
Lo stadio B2 di Tanner
(bottone mammario)
segna l'inizio dello
sviluppo puberale nella
femmina
Nel maschio un volume
testicolare > 4 ml o
diametro > 2.5 cm segna
l'inizio della pubertà
SI
oz
8
01
orchidometro di
Prader
25
4
6
5
2PUBERTA' PRECOCE
Definizione di pubertà precoce
Comparsa dei caratteri sessuali secondari ad un'età < - 2 SDS rispetto
alla media della popolazione generale (prima dell'età di 8 anni nelle
femmine e dei 9 anni nel maschio)
-2 SD
-1 SD Mean +1 SD +2 SD
-
1
Precocious
Puberty
F>> M
Delayed
Puberty
M >> F
Number
of
Children
I
eg.
eg.
Hypothalamic
Hamartoma
Inflammatory
Bowel Disease
Age at Onset of Puberty
- E' una condizione relativamente rara
- Incidenza di 1/5.000-1/10.000
- Più comune nelle femmine, con
rapporto femmine maschi che varia da
3:1 a 23:1
Berberogluetal, J Clin Ped Endo 2009B
Stadiazione della pubertà secondo Marshall e Tanner
STADIO B1
STADIO G1
testicoli < 4 ml
STADIO B2
11,8 anni
(8,9-13,2 anni)
STADIO G2
11,6 anni - testicoli 4-6 ml
(9,5-13,8 anni)
STADIO B3
12,1 anni
(10-14,3 anni)
Pubarca V
STADIO G3
12,8 anni - testicoli > 6 <10 ml
(10,8-14,9 anni)
Spermarca
13,4 anni - testicoli 12 ml
(11,7-15,3)
STADIO G4
13,8 anni - testicoli 10-15 ml
Pubarca V
(11,7-15,8 anni)
STADIO B5
15,3 anni
(11,8-18,8 anni)
STADIO G5
14,9 anni - testicoli > 15 ml
(12,7-17,1 anni)
FIGURA 3 Stadiazione della pubertà secondo Marshall e Tanner (età media ± 2 DS).
(Modificata dall'Autore da (A) Marshall e Tanner, Arch Dis Child 1969 e da (B) Marshall e Tanner,
Arch Dis Child 1970)4,5
Segni clinici di pubertà precoce
V
Sviluppo mammario (Tanner B2 o >) in bambine < 8 aa o
incremento volume testicolare (> 4ml) in bambini < 9 aa
V
Aumento velocità di crescita
V
Avanzamento dell'età ossea
v Comparsa di peluria pubica (e ascellare)
/ Segni aggiuntivi (perdite vaginali; acne, capelli grassi, erezioni e
polluzioni notturne)
V Aumento delle dimensioni ovariche e uterine all'ecografia pelvica
V
Aumento livelli di LH basale e/o dopo test di stimolo con GnRH
1
Possibili alterazioni RMN encefalo (ipotalamo-ipofisi)
PUBERTA' PRECOCE
STADIO B4
13,1 anni
(10,8-15,3 anni)HORMONE
RESEARCH IN
PÆDIATRICS
Mini Review
Horm Res Paediatr 2012;77:137-145
DOI: 10.1159/000336325
Recent Secular Trends in Pubertal Timing
Implications for Evaluation and Diagnosi!
of Precocious Puberty
Kaspar Sørensen Annette Mouritsen Lise Aksglaede Casper P. Hagen
Signe Sloth Mogensen Anders Juul
Department of Growth and Reproduction, Rigshospitalet, Faculty of Health Sciences, University of Copenhagen,
Copenhagen, Denmark
Anticipazione dello sviluppo puberale
18
14.0
Denmark
13.5
- Portugal
13.0
- Norway
16
12.5
US
1970
1980
1990
2000
- Germany
15
Year of study
Finland
14
Spain
-
Greece
13
Netherlands
- Belgium
12
Poland
1830 1850 1870 1890 1910 1930 1950 1970 1990 2010
Year of study
PUBERTA'
Anticipazione inizio sviluppo puberale registrato nei
paesi industrializzati
Fenomeno più evidente nel
sesso femminile
Teorie sull'anticipazione puberale
Teorie:
-Alimentazione (obesità)
Kaplowitzetal, Pediatrics 2009
-Alimentazione in gravidanza
-Attività fisica
- Interferenti endocrini
(endocrine disruptors)
- ecc
Age at menarche
17
Age at menarche (years)
(years)Incidenza PPC: non adottati vs adottati
Pubertà precoce e fattori ambientali
Human Reproduction Vol.16, No.5 pp. 1020-1026, 2001
Sexual precocity after immigration from developing
countries to Belgium: evidence of previous exposure to
organochlorine pesticides
M.Krstevska-Konstantinova1,7, C.Charlier2, M.Craen3, M.Du Caju4, C.Heinrichs5,
C.de Beaufort6, G.Plomteux2 and J.P.Bourguignon1,8
1Division of Ambulatory Pediatrics and Adolescent Medicine, Department of Pediatrics and 2Laboratory of Toxicology, University of
Liège, C.H.U. Sart Tilman, Liège, Belgium and Departments of Pediatrics, Universities of 3Ghent, 4Antwerp, 5Brussels and 6Centre
Hospitalier de Luxembourg, in collaboration with the Belgian Study Group for Pediatric Endocrinology
7Present address: Pediatric Clinic, Medical Faculty, 91000 Skopje, Macedonia
8To whom correspondence should be addressed at: Division of Ambulatory Pediatrics and Adolescent Medicine, University of Liège,
C.H.U. Sart Tilman, B-4000 Liege, Belgium. E-mail: jpbourguignon@ulg.ac.be
In a retrospective auxological study of 145 patients seen in Belgium during a 9-year period for treatment of
precocious puberty, 28% appeared to be foreign children (39 girls, one boy) who immigrated 4 to 5 years earlier
from 22 developing countries, without any link to a particular ethnic or country background. The patients were
either adopted (n = 28) or non-adopted (n = 12), the latter having normal weight and height at immigration and
starting early puberty without evidence of earlier deprivation. This led to the hypothesis that the mechanism of
precocious puberty might involve previous exposure to oestrogenic endocrine disrupters. A toxicological plasma
screening for eight pesticides detected p,p'-DDE, which is derived from the organochlorine pesticide DDT. Median
Possibili cause di pubertà precoce
Possibili cause:
· Migliori condizioni
ambientali (nutrizione,
igiene, ecc.)
· Migliore "ambiente"
psico-affettivo
· Possibile effetto degli
"endocrine disrupters"
Krstevka-Konstantinova, Human Repr 2001ARTICLES | AUGUST 01 2006
Increased Risk of Precocious Puberty in Internationally Adopted
Children in Denmark !!
Grete Teilmann, MD; Carsten B. Pedersen, MSc; Niels E. Skakkebæk, MD, PhD; Tina Kold Jensen, MD, PhD
PEDIATRICS®
Registro nazionale Danese 1983-2001 -> 655 casi di CPP:
b.ni adottati hanno un rischio di PPC > di 15-20 volte rispetto ai coetani danesi
Fattori psicosociali di stress, presenti nei b.ni adottati, possono impattare sulla
maturazione puberale
Non aumento di PPC in b.ni immigrati con le loro famiglie che conservano le loro
abitudini sociali e alimentari dopo l'immigrazione
Una più elevata età di adozione aumenta il rischio di PPCPUBERTA' PRECOCE
Classificazione della pubertà precoce
CENTRALE (vera o gonadotropina dip.)
PERIFERICA (peudoPP o gonadotropina
indip.)
- Incidenza 1:5.000/10.000
- M:F = 1:15-20; > rischio in adottati
- Isosessuale
- Più frequentemente idiopatica (F
90%); > incidenza di cause
organiche nel maschio - Molto meno frequente
- Isosessuale/eterosessuale
- Segni clinici a comparsa più rapida,
sequenza incompleta o atipica - Trattamento a seconda della causaCAUSE DI PUBERTA' PRECOCE
Cause di pubertà precoce centrale
CENTRALE (vera o gonadotropina dip.)
- Idiopatica (70-80%)
- Neoplasie del SNC
(astrocitoma, glioma ottico,
amartroma ipotalamico,
craniofaringioma ... ) (15-20%) - Altre lesioni del SNC (ascesso,
encefalite, trauma, idrocefalo,
radioterapia, chemioterapia ... )
(5-10%) - Genetica: mutazione dei geni
KISS1, KISS1R ...
Cause di pubertà precoce periferica
PERIFERICA (peudoPP o gonadotropina
indip.)
- Gonadica: sindrome di McCune
Albright, mutazione attivante il
recettore per l'LH, tumori ovarici,
tumori a cellule di Leydig - Surrenalica: sindrome adreno genitale,
iperplasia surrenalica congenita,
adenoma/carcinoma surrenalico - Tumori producenti gonadotropina
corionica umana (HCG) - Altre: iatrogena (steroidi),
ipotiroidismo primario, endocrine
distruptorsPUBERTA' PRECOCE E GENETICA
Genetica della pubertà precoce
Sono state identificate mutazioni in quattro geni distinti in pazienti e famiglie con PPC: KISS1, KISSR (kisspeptin
receptor), MKRN3 (makorin ring finger protein 3), DLK1 (Delta-like non canonical Notch ligand 1)
Genetic causes of CPP
Preoptic area
1
KISS1
Hypothalamus
Kisspeptin neuron
3
MKRN3
1
3
?
3 ?
4 DLK1
4
?
4
?
Arcuate nucleus
GnRH neuron
KISS1R
KNDy neuron
2
2
KISS1R
Median eminence
GnRH
Anterior pituitary gland
Posterior pituitary gland
Gonad
LH
FSH
Sex steroids
Gametogenesis
Da Roberts, Kaiser; European Journal of Endocrinology 2020
Cause genetiche confermate e potenziali
Table 2
Known and potential genetic causes of central precocious puberty.
Gene
Protein
Function
Reference
Confirmed Causes of Central Precocious Puberty
KISS1
Kisspeptin
KISS1R
Binds to KISS1 receptor
[14,66]
KISS1R
G protein-couple receptor, involved in increased
GnRH pulsatility
[13,67]
MKRN3
MKRN3
DLK1
Delta-like homolog 1
Ubiquitinylation, cell signaling
Pituitary cell differentiation
[16,17,68-70]
[20]
Potential Causes of Central Precocious Puberty that have not yet been validated in humans
GABRA1
Gamma amino butyric acid A1 receptor
a-1 subunit
LIN28B
Lin 28 homolog B
Unknown, homolog of C. elegans protein involved
in GnRH secretion
[2,7,27]
NPYR
Neuropeptide Y
[2,7,27]
TAC3 &
Neurokinin B (NKB) & NKBR
TACR3
NKB
NK3R
- leptin
kisspeptin
GnRH neuron
2
KISSIP
MKRN3
Nptx1
MKRN3
GnRH pulses
GnRH pulses
Pituitary
* DLK1
A. Puberty
B. Prepubertal
Fig. 1. A schematic illustrating some of the key players in puberty initiation. A. Potential roles in puberty initiation. Neurokinin
B (NKB) and its receptor NK3R induce GnRH pulses, likely though increased kisspeptin levels. Nptx levels increase during puberty
and its levels are inversely associated with MKRN3, although the exact role is still unknown. * Denotes genes in which mutations
have been described in individuals with CPP. B. Prepubertal. The GnRH pulses are largely suppressed. Nptx1 levels are low due to
ubiquitinylation by MKRN3, which results in Nptx1 degradation.
R.S. Aguirre, E.A. Eugster, Best Practice & Research Clinical
Endocrinology & Metabolism 2018
GnRH neuron
Nptx1 degradation
KISSIR
Nptx1
[7]
insulin
Puberty acceleration via kisspeptin
[7]
Antagonizes GABA effects on GnRH neurons
Regulation of GnRH secretion
1
2
KISS1RREVIEW
OPEN ACCESS
Hypothalamic Hamartomas
Evolving Understanding and Management
Nathan T. Cohen, MD, J. Helen Cross, MB ChB, PhD, Alexis Arzimanoglou, MD, Samuel F. Berkovic, MD,
John F. Kerrigan, MD, Ilene Penn Miller, JD, LLM, Erica Webster, Lisa Soeby, MBA, Arthur Cukiert, MD, PHD,
Dale K. Hesdorffer, PhD, Barbara L. Kroner, PhD, Clifford B. Saper, MD, PhD, Andreas Schulze-Bonhage, MD, PhD,
and William D. Gaillard, MD, on behalf of the Hypothalamic Hamartoma Writing Group
Neurology® 2021;97:864-873. doi:10.1212/WNL.0000000000012773
Amartoma ipotalamico
Tumore benigno (neuroni e cellule della glia), raro (1/100.000,
M>F: 1.3 vs1), congenito (si forma durante periodo fetale)
Due variant anatomiche:
ü
Intraipotalamico (o sessile): connesso con l'ipotalamo
posteriore e terzo ventricolo (vicino ai corpi mammillari) >
associato a crisi gelastiche (risata ictale) o dacristiche (pianto
ictale)
ü
Paraipotalamico (o penduncolato): vicino ipotalamo anteriore,
tuber cinereum, peduncolo ipofisario, e attaccato al
pavimento del III ventricolo > associato a PPC
- 95% sporadico (20% associato a mut gene GLI3 somatiche)
- 5% associato a Snd di Pallister-Hall (mut gene GLI3):
dismorfismi mani e piedi (polidattilia e sindattilia), epiglottide
bifida, anomalie ano e ipotalamo
Amartoma
Ipotalamico
più frequente causa
lesionale di PPC
A
B
Fig. 1 -(A) T2-weighted coronal image demonstrates a well-defined, lobulated lesion arising from the tuber cinereum and
extending into the third ventricle (solid white arrows) with iso- to high signal intensity. (B) T1-weighted axial image
demonstrates the extension of the lesion into the interpeduncular cistern and it abuts the optic radiation bilaterally (white
dashed arrows)
A
B
Fig. 2 - (A) T1-weighted sagittal image shows the lesion projecting into the suprasellar (solid white arrow) and pre-pontine
(dashed white arrow) cisterns. (B) Post-contrast sagittal image shows non-enhancing hypothalamic hamartoma (solid white
arrow)
Non hai trovato quello che cercavi?
Esplora altri argomenti nella Algor library o crea direttamente i tuoi materiali con l’AI.
