Respiratory Physiology Lecture 6: Control of Respiration and Muscles
Slides about Respiratory Physiology Lecture 6. The Pdf explores respiratory physiology, focusing on the muscles involved in breathing and the nervous control of the process. This University Biology Pdf details the role of the respiratory center in the brainstem, including medullary, pneumotaxic, and apneustic areas.
See more11 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Control of Respiration Muscles
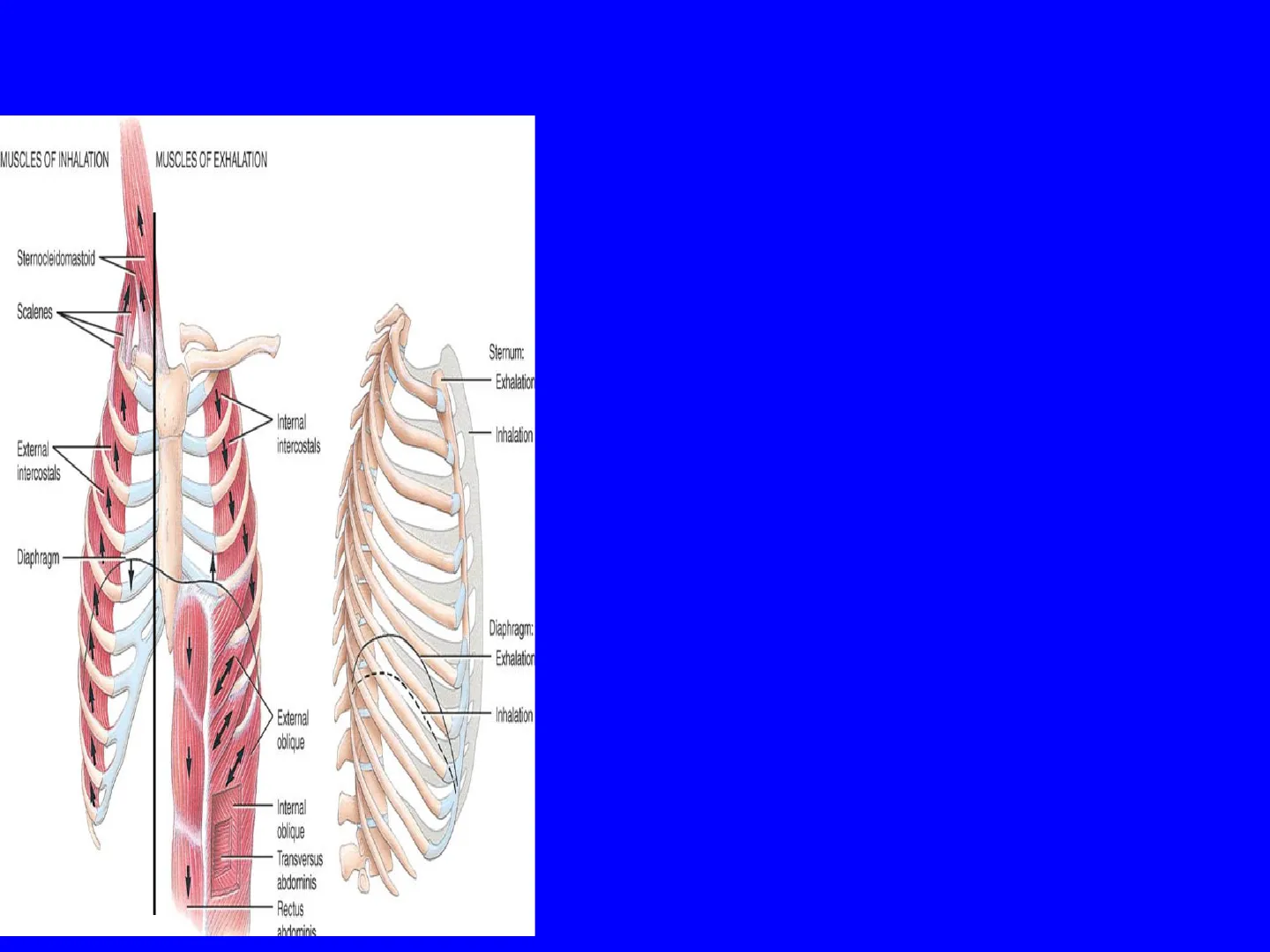
Muscles of Inhalation and Exhalation
MUSCLES OF INHALATION
MUSCLES OF EXHALATION
Sternocleidomastoid
Scalenes
Sternum:
Exhalation
Internal
intercostals
- Inhalation
External
intercostals
Diaphragm
Diaphragm:
Exhalation
Inhalation
External
oblique
- Internal
obliqu
Transversus
abdominis
Rectus
abdominis
- Quiet inhalation; The most important muscle of inhalation is the diaphragm, a dome shaped muscle, that forms the floor of the thoracic cavity. Contraction of the diaphragm causes it to flatten and increase the vertical height of the thoracic cavity. During normal quiet inhalation the diaphragm descends about 1 cm, producing a pressure difference of 1- 3 mm Hg and the inhalation of about 500 ml of air. The contraction of the diaphragm is responsible for 75% of inhaled air. The other muscles that are involved are the external intercostal muscles. When these muscles contract they elevate the ribs, and increase the width and depth of the thoracic cavity. The external intercostal muscles are responsible for about 25% of the air entering the lungs.
- Inhalation during strenuous exercise; In strenuous breathing the diaphragm may descend 10 cm, which produces a pressure difference of 100 mm Hg and the inhalation of 2-3 litres of air. During deep, forceful , inhalations, the accessory muscles of inspiration participate in increasing the volume of the thoracic cavity. The accessory muscles are the sternocleidomastoideoles that elevate the sternum, the scalene muscles that elevate the first two ribs, and the pectoralis minor muscles that elevate the 3-5th ribs. Both normal quiet inhalation and inhalation during exercise involve muscle contraction and are therefore active processes.
- Advanced pregnancy, excessive obesity or confining abdominal clothing can prevent complete descent of the diaphragm.
Role of the Respiratory Center
The size of the thorax is altered by respiratory muscles that contract in response to signals transmitted from nerve centres in the brain stem, and relax in the absence of impulses. The muscles are under control of a dispersed group of neurons, collectively called the respiratory centre, which can be divided into 3 areas on the basis of their function;
- the medullary rhythmicity centre in the medulla oblongata
- the pneumotaxic area in the pons
- the apneustic area also in the pons
Respiratory Center Sagittal Plane
Sagittal
plane
RESPIRATORY
CENTER:
Midbrain
Pneumotaxic area
Apneustic area
Pons
Medullary rhythmicity
area:
Inspiratory area
Medulla
oblongata
Expiratory area
Spinal
cord
Sagittal section of brain stem
O Ventilation is controlled by neurons in pons & medulla oblongata in the brain
3 groups of neurons
- medullary rhythmicity area in the medulla oblongata
- pneumotaxic area in the pons
- apneustic area in the pons
Medullary Rhythmicity Area
Activates
INSPIRATORY AREA
ACTIVE
INACTIVE
INSPIRATORY AREA
ACTIVE
EXPIRATORY AREA
2 seconds
3 seconds
Diaphragm and external
intercostals actively
contract
Diaphragm and external
intercostals relax, followed
by elastic recoil of chest
wall and lungs
Diaphragm,
sternocleidomastoid
and scalene muscles
contract
Internal intercostal
and abdominal
muscles contract
active
active
passive
active
Normal quiet inhalation
Normal quiet exhalation
Forceful inhalation
Forceful exhalation
(a) During normal quiet breathing
(b) During forceful breathing
- Controls basic rhythm of respiration
- Normal quiet breathing the expiratory area is inactive . During forceful breathing the inspiratory area activates the expiratory area, which is active during high ventilation rates
The function of the medullary rhythmicity area is to control the basic rhythm of respiration. There are inspiratory and expiratory areas within the medullary rhythmicity area. The figure shows the relationship between these two areas during normal quiet breathing and forceful breathing. During quiet breathing the inspiratory area generates nerve impulses for about 2 seconds which are transmitted via nerves to the external intercostal muscles and the diaphragm, causing them to contract and inhalation to occur. This is therefore an active process. After 2 seconds the inspiratory centre becomes inactive and the external intercostal muscles and diaphragm relax for about 3 seconds in the passive process of exhalation. Exhalation is also due to the elastic recoil of alveolar walls.
- The neurons of the expiratory centre remain inactive during quiet breathing. However, during forceful breathing impulses from the inspiratory area activate the expiratory area. Impulses from the expiratory area thencause contraction of the internal intercostal muscles and the abdominal muscles to cause forceful exhalation, for example during exercise or playing a wind instrument. The inspiratory centre is regulated by other sites in the brain stem, the pneumotaxic area and the apneustic area, which alter the rate of transition from inhalation to exhalation and therefore the rate of breathing.
Role of the Respiratory Center: Pneumotaxic Area
The pneumotaxic
area sends inhibitory
impulses to the
inspiratory area
Sagittal
plane
RESPIRATORY
CENTER:
Midbrain
Pneumotaxic area
Apneustic area
Pons
- Medullary rhythmicity
area:
Inspiratory area
Medulla
oblongata
Expiratory area
Spinal
cord
These signals
shorten the duration
of inhalation.
Sagittal section of brain stem
Role of the Respiratory Center: Apneustic Area
The apneustic area
sends stimulatory
impulses to the
inspiratory area
Sagittal
plane
RESPIRATORY
CENTER:
Midbrain
Pneumotaxic area
Apneustic area
Pons
+ Medullary rhythmicity
area:
Inspiratory area
Medulla
oblongata
Expiratory area
These signals
prolong the duration
of inhalation.
Spinal
cord
Sagittal section of brain stem
Chemical Regulation of Respiration
- Central chemoreceptors in medulla oblongata detect changes in CSF, PCO2 and H+
- Peripheral chemoreceptors - in carotid bodies detect changes in PO2, PCO2 and H+ - in aortic bodies detect changes in PO2, PCO2 and H+
Chemoreceptors and Nerve Impulses
Medulla oblongata
1
1
Sensory axons in
glossopharyngeal nerve
(cranial nerve IX)
Internal carotid
artery
Carotid
body
External carotid
artery
Carotid sinus
Common carotid
artery
Sensory axons
in vagus nerve
(cranial nerve X)
1
Arch of aorta
Aortic bodies
Heart
Notes on Chemoreceptors
NOTES
- Central chemoreceptors are found in the medulla oblongata of the brain stem, and respond to changes in PCO2 and H+ in the cerebrospinal fluid.Peripheral chemoreceptors are located in the aortic bodies and in the carotid bodies. They detect changes in PO2, PCO2 and H+ .
- Aortic bodies are found in the wall of the arch of the aorta. Carotid bodies are found in the left and right carotid arteries. In both cases they are located close to the baroreceptors that detect blood pressure. Sensory nerves from the peripheral chemoreceptors send impulses to the respiratory centre.
- CO2 is lipid soluble and readily enters cells where it combines with water and in the presence of carbonic anhydrase generates carbonic acid, which subsequently dissociates to H+ and HCO3 -. The resulting increase in H+ is detected following even a very small change in PCO2 from the normal value in arterial blood of 40 mm Hg. An increase in PCO2 in arterial blood is called hypercapnia. Hypercapnia is detected by both central and peripheral chemoreceptors. . However, in addition, the peripheral chemoreceptors can also detect and respond to a deficiency in O2. When PO2 in arterial blood falls below a normal value of 100 mm Hg, but is still above 50 mm Hg, the peripheral chemoreceptors are stimulated. . However, if PO2 falls below 50 mm Hg, the severe deficiency in 02 suppresses the activity of central chemoreceptors and the inspiratory area, which then do not respond well and send fewer impulses for inspiration. As the respiratory rate falls and PO2 falls lower and lower, a positive feedback cycle is established with fatal results.
Chemoreceptor Regulation of Respiration
- A slight increase in Pco2 (and thus H+), a condition called hypercapnia, stimulates central and peripheral chemoreceptors
- As a response to increased Pco2, increased H+ and decreased PO2, the inspiratory area is activated and hyperventilation, rapid and deep breathing, occurs is lower than 40 mm Hg, a condition . If arterial Pco2 called hypocapnia, the chemoreceptors are not stimulated and the inspiratory area sets its own pace until CO2 accumulates and Pco2 rises to 40 mm Hg.
- Severe deficiency of O2 depresses activity of the central chemoreceptors and respiratory center
Negative Feedback Regulation of Breathing
Some stimulus disrupts
homeostasis by
Increasing
Arterial blood Pco2
(or decreasing pH or Po2)
Receptors
Central
chemo-
Peripheral
chemo-
receptors receptors
in
medulla
in aortic
and
carotid
bodies
Input
Nerve
impulses
Control center
Inspiratory area in
medulla oblongata
Output
Nerve
impulses
Effectors
Muscles of
inhalation and
exhalation
contract more
forcefully and
more frequently
(hyperventilation)
Decrease in arterial
blood Pco2, increase in
pH, and increase in Po2
Return to homeostasis
when response brings
arterial blood Pco2, PH,
and Po2 back to normal
Negative feedback
regulation of breathing
- Negative feedback control of breathing
- Increase in arterial pCO2
- Stimulates chemoreceptors
- Sensory nerves send signals to the inspiratory center
- Muscles of respiration contract more frequently & forcefully
- pCO2 Decreases
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
