PCOS, Hirsutism and Female Sexuality: Definitions, Signs, and Symptoms
Document from Prof. Greco about PCOS, Hirsutism and Female Sexuality. The Pdf explores the polycystic ovary syndrome, hirsutism, and female sexuality, presenting definitions, signs, and symptoms, including menstrual disorders and sexual pain, for university-level Biology students.
See more22 Pages

Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
PCOS: Polycystic Ovary Syndrome
Page 1 of 22
OB/GYN - Prof. Greco - PCOS and Female Sexuality
Obstetrics and Gynecology
PCOS, hirsutism and female sexuality
Prof. Greco - 27/03/24
Autore: Beya Latrous
Revisore: Lorena Corigliano
1. PCOS: Polycystic ovary syndrome
Polycystic ovary syndrome (PCOS) is the
most common endocrine disorder in women
of reproductive age.
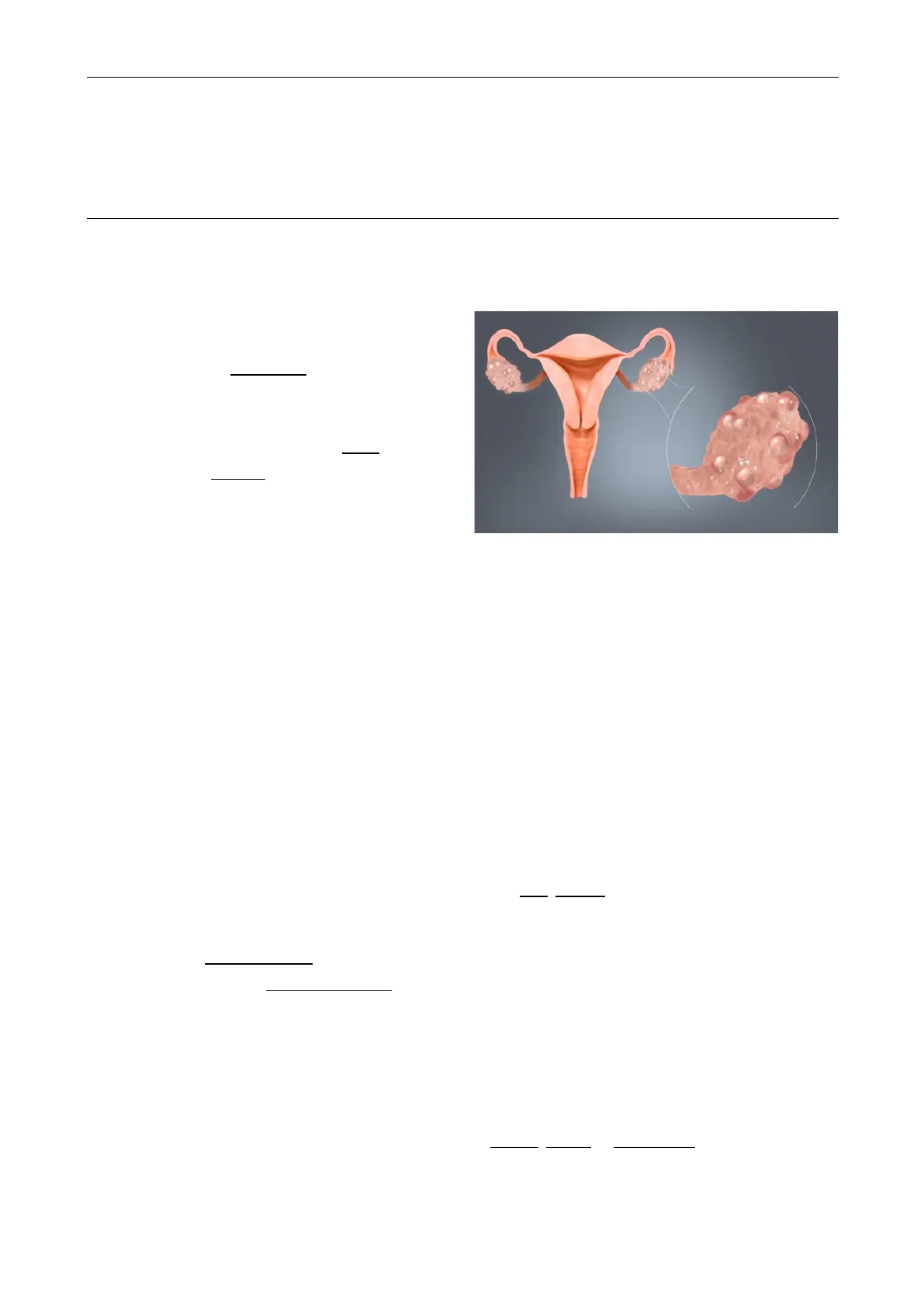
The syndrome is named after cysts which
form on the ovaries of some people with this
condition, though this is not a universal
symptom, and not the underlying cause of
the disorder.
The prevalence of PCOS could be as high as 26% among some populations > though ranges
between 4% and 18% are reported for general populations.
The exact cause of PCOS remains uncertain, and treatment involves management of symptoms
using medication.
PCOS Definition
1.1 Definition
Three definitions are commonly used:
1) NIH
In 1990, a consensus workshop sponsored by the NIH/NICHD suggested that a person has
PCOS if they have :
- oligoovulation
- signs of androgen excess (clinical or biochemical)
- exclusion of other disorders that can result in menstrual irregularity and
hyperandrogenism (e.g .: Congenital Suprarrenal Hyperplasia, androgen producer
tumors, hyperprolactinemia).
2) Rotterdam
In 2003, a consensus workshop sponsored by ESHRE/ASRM in Rotterdam indicated PCOS to
be present if any two out of three criteria are met, in the absence of other entities thatPage 2 of 22
OB/GYN - Prof. Greco - PCOS and Female Sexuality
might cause these findings:
- oligoovulation and/or anovulation
- excess androgen activity
- polycystic ovaries (by gynecologic ultrasound)
> The Rotterdam definition is wider, including many more women, the most notable
ones being women without androgen excess. Critics say that findings obtained from the
study of women with androgen excess cannot necessarily be extrapolated to women
without androgen excess.
3) Androgen Excess PCOS Society
In 2006, the Androgen Excess PCOS Society suggested a tightening of the diagnostic criteria
to all of the following:
- excess androgen activity
- oligoovulation/anovulation and/or polycystic ovaries
- exclusion of other entities that would cause excess androgen activity
Signs and Symptoms of PCOS
1.2 Signs and symptoms
1) Menstrual disorders
PCOS mostly produces oligomenorrhea (fewer than nine menstrual periods in a year)
or amenorrhea (no menstrual periods for three or more consecutive months), but other
types of menstrual disorders may also occur.
2) Infertility: generally results directly from chronic anovulation (lack of ovulation).
3) High levels of masculinizing hormones: known as hyperandrogenism, the most common
signs are acne and hirsutism , but it may produce hypermenorrhea (heavy and prolonged
menstrual periods), androgenic alopecia (increased hair thinning or diffuse hair loss), or
other symptoms. Approximately three-quarters of women with PCOS have evidence
of hyperandrogenemia.
4) Metabolic syndrome: this appears as a tendency towards central obesity and other
symptoms associated with insulin resistance, including low energy levels and food cravings.
> Serum insulin, insulin resistance, and homocysteine levels are higher in women with
PCOS.Page 3 of 22
OB/GYN - Prof. Greco - PCOS and Female Sexuality
5) Acne: A rise in testosterone levels, increases the oil production within the sebaceous
glands and clogs pores. For many people, the emotional impact is great and quality of life
can be significantly reduced.
6) Androgenic Alopecia: Estimates suggest that androgenic alopecia affects 22% of PCOS
sufferers. This is a result of high testosterone levels that are converted into the
dihydrotestosterone (DHT) hormone. Hair follicles become clogged, making hair fall out
and preventing further growth.
7) Acanthosis Nigricans (AN): A skin condition where dark, thick and "velvety" patches can
form.
8)
Polycystic ovaries: ovaries might get enlarged and comprise follicles surrounding the eggs.
As result, ovaries might fail to function regularly.
This disease is related to the number of follicles per ovary each month growing from the
average range of 6-8 to double, triple or more
> women with PCOS have higher risk of multiple diseases including Infertility, type 2
diabetes mellitus (DM-2), cardiovascular risk, metabolic syndrome, obesity, impaired
glucose tolerance, depression, obstructive sleep apnea (OSA), endometrial cancer, and
nonalcoholic fatty liver disease/nonalcoholic steatohepatitis (NAFLD/NASH).
Women with PCOS tend to have central obesity. In fact whether visceral and subcutaneous
abdominal fat is increased, unchanged, or decreased in women with PCOS relative to non-
PCOS women with the same body mass index.
Androgens, such as testosterone, dihydrotestosterone, and nandrolone decanoate have been
found to increase visceral fat deposition in both female animals and women
Although 80% of PCOS presents in women with obesity, 20% of women diagnosed with the
disease are non-obese or "lean" women.
However, obese women that have PCOS have a higher risk of adverse outcomes, such as:
- hypertension
- insulin resistance
- metabolic syndrome
- endometrial hyperplasia
Even though most women with PCOS are overweight or obese, it is important to acknowledge
that non-overweight women can also be diagnosed with PCOS.Page 4 of 22
OB/GYN - Prof. Greco - PCOS and Female Sexuality
Up to 30% of women diagnosed with PCOS maintain a normal weight before and after
diagnosis.
Lean women are likely to have a missed diagnosis of diabetes and cardiovascular disease.
These women also have an increased risk of developing insulin resistance, despite not being
overweight. Lean women are often taken less seriously with their diagnosis of PCOS, and also
face challenges finding appropriate treatment options-> This is because most treatment
options are limited to approaches of losing weight and healthy dieting.
Hormone Levels in PCOS
1.3 Hormone levels
Testosterone Levels in PCOS
1.3.1 Testosterone
Testosterone levels are usually elevated in women with PCOS.
In a 2020 systematic review and meta-analysis of sexual dysfunction related to PCOS
(5,366 women with PCOS from 21 studies) testosterone levels were analyzed and were
found to be:
= 2.34 nmol/L (67 ng/dL) in women with PCOS
= 1.57 nmol/L (45 ng/dL) in women without PCOS.
In a 1995 study of 1,741 women with PCOS, mean testosterone levels were 2.6 (1.1-4.8)
nmol/L (75 (32-140) ng/dL).
In a 1998 study which reviewed many studies and subjected them to meta-analysis,
testosterone levels in women with PCOS were 62 to 71 ng/dL (2.2-2.5 nmol/L) and
testosterone levels in women without PCOS were about 32 ng/dl (1.1 nmol/L).
In a 2010 study of 596 women with PCOS which used liquid chromatography-mass
spectrometry (LC-MS) to quantify testosterone, median levels of testosterone were 41 and
47 ng/dL (with 25th-75th percentiles of 34-65 ng/dl and 27-58 ng/dl and ranges of 12-
184 ng/dl and 1-205 ng/dL) via two different labs.
If testosterone levels are above 100 to 200 ng/dl, other possible causes
of hyperandrogenism, such as congenital adrenal hyperplasia or an androgen-
secreting tumor, may be present and should be excluded.
LH-FSH Ratio in PCOS
1.3.2 LH-FSH
In women with PCOS, the ratio of Luteinizing Hormone (LH) to Follicle-Stimulating
Hormone (FSH) is typically elevated, ranging from 2 to 3; whereas in healthy women, itPage 5 of 22
OB/GYN - Prof. Greco - PCOS and Female Sexuality
typically stays within the range of 1 to 2.
This imbalance is driven by an increase in luteinizing hormone levels and a decrease in
follicle-stimulating hormone levels.
Associated Conditions with PCOS
1.4 Associated conditions
Warning signs may include a change in appearance. But there are also manifestations of
mental health problems such as anxiety, depression and eating disorders.
A diagnosis of PCOS suggests an increased risk of the following:
- Endometrial hyperplasia and endometrial cancer (cancer of the uterine lining) are
possible, due to overaccumulation of uterine lining, and also lack of progesterone,
resulting in prolonged stimulation of uterine cells by estrogen. - Insulin resistance/type 2 diabetes. A review published in 2010 concluded that women
with PCOS have an elevated prevalence of insulin resistance and type 2 diabetes, even
when controlling for body mass index (BMI).PCOS is also associated with higher risk for
diabetes. - High blood pressure, in particular if obese or during pregnancy
- Depression and anxiety
- Dyslipidemia disorders of lipid metabolism, cholesterol and triglycerides. Women with
PCOS show a decreased removal of atherosclerosis-inducing remnants, seemingly
independent of insulin resistance/type 2 diabetes. - Cardiovascular disease, with a meta-analysis estimating a 2-fold risk of arterial disease for
women with PCOS relative to women without PCOS, independent of BMI. - Strokes
- Weight gain
- Miscarriage
- Sleep apnea, particularly if obesity is present
- Non-alcoholic fatty liver disease, particularly if obesity is present
- Acanthosis nigricans (patches of darkened skin under the arms, in the groin area, on the
back of the neck) - Autoimmune thyroiditis
- Iron deficiency
- The risk of ovarian cancer and breast cancer is not significantly increased overallPage 6 of 22
OB/GYN - Prof. Greco - PCOS and Female Sexuality
Causes of PCOS
1.5 Causes
PCOS is an heterogeneous disorder of uncertain cause.
There is some evidence that it is a genetic disease and such evidence includes
- the familial clustering of cases,
- greater concordance in monozygotic compared with dizygotic twins
- heritability of endocrine and metabolic features of PCOS.
There is some evidence that exposure to higher than typical levels of androgens and the anti-
Müllerian hormone (AMH) in utero increases the risk of developing PCOS in later life.
It may be caused by a combination of genetic and environmental factors.
Risk factors include:
- obesity
- lack of physical exercise,
- family history
Diagnosis is based on two of the following 3 findings:
- anovulation
- high androgen levels
- ovarian cysts-> cysts may be detectable by ultrasound.
Other conditions that produce similar symptoms include
- adrenal hyperplasia
- hypothyroidism
- high blood levels of prolactin
Genetics of PCOS
1.5.1 Genetics
The genetic component appears to be inherited in an autosomal dominant fashion with
high genetic penetrance but variable expressivity in females.
This means that each child has a 50% chance of inheriting the predisposing genetic
variant(s) from a parent, and, if a daughter receives the variant(s), the daughter will have
the disease to some extent.
The genetic variant can be inherited from either the father or the mother, and can be
passed along to both sons (who may be asymptomatic carriers or may have symptoms such
as early baldness and/or excessive hair) and daughters, who will show signs of PCOS.
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
