Rheumatoid Arthritis: Aetiology and Inflammatory Response, University of Portsmouth
Slides from University of Portsmouth about Rheumatoid Arthritis: Aetiology and Inflammatory Response. The Pdf explores the classification of autoimmune diseases and the mechanisms of T lymphocyte selection in the thymus and periphery, relevant for University Biology students.
See more22 Pages


Unlock the full PDF for free
Sign up to get full access to the document and start transforming it with AI.
Preview
Learning Objectives
On completion of this session you should be able to
- Describe what systemic autoimmune diseases are and provide an overview of their characteristics.
- Explain the pathophysiology and clinical features of Rheumatoid Arthritis (RA).
Autoimmune Classification
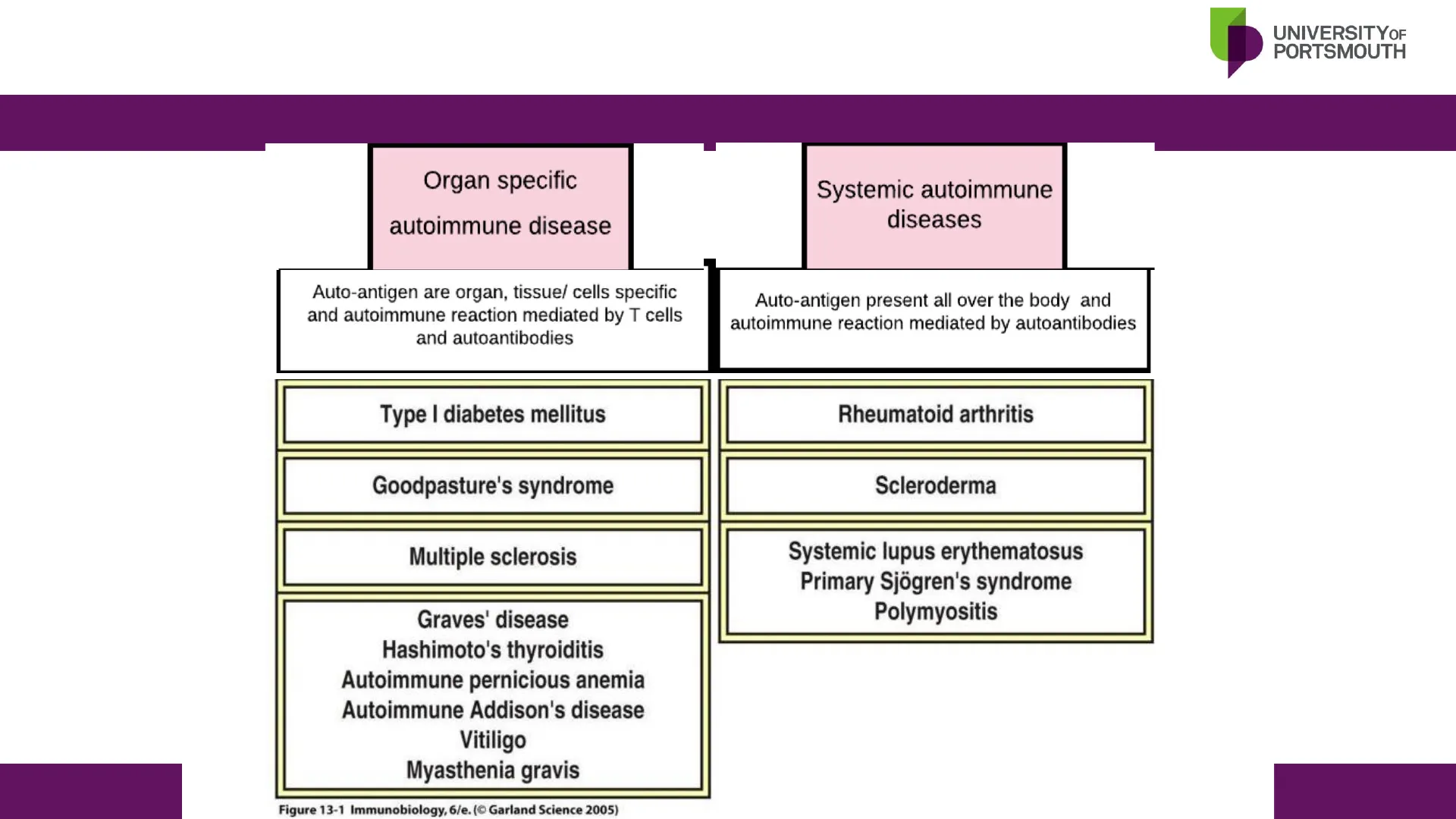
Organ-Specific vs. Systemic Autoimmune Diseases
Organ specific autoimmune disease
Systemic autoimmune diseases
Auto-antigen are organ, tissue/ cells specific and autoimmune reaction mediated by T cells and autoantibodies
Auto-antigen present all over the body and autoimmune reaction mediated by autoantibodies
Type I diabetes mellitus Rheumatoid arthritis Goodpasture's syndrome Scleroderma Multiple sclerosis Graves' disease Hashimoto's thyroiditis Autoimmune pernicious anemia Autoimmune Addison's disease Vitiligo Myasthenia gravis Systemic lupus erythematosus Primary Sjogren's syndrome Polymyositis
Figure 13-1 Immunobiology, 6/e. (@ Garland Science 2005)
Systemic Autoimmune Disease Pathogenic Mechanisms
- Autoantibodies: Bind autoantigen to form autoantigen-antibody complexes, which cause tissue damage due to activation of complement, inflammation and activation of Fc-receptor systems.
Systemic autoimmune diseases are characterized by the immune system's aberrant response against the body's own tissues, leading to widespread inflammation and organ damage. The pathogenic mechanisms underlying these diseases involve complex interactions between genetic predispositions and environmental triggers. A hallmark feature is the production of autoantibodies, which recognize and bind to self-antigens, forming immune complexes. These immune complexes can deposit in various tissues, triggering the activation of the complement system.
The subsequent complement cascade promotes inflammation and recruits immune cells, such as macrophages and neutrophils, to the site of deposition. Furthermore, autoantibodies can engage Fc receptors on these immune cells, enhancing their inflammatory responses and leading to tissue damage. Cytokines released by activated immune cells perpetuate the inflammatory cycle, causing chronic tissue injury. This multifaceted immune response underlies the pathology of systemic autoimmune diseases like systemic lupus erythematosus (SLE), where diverse organs including the kidneys, skin, and joints can be affected, manifesting in a wide array of clinical symptoms.
Rheumatoid Arthritis Characteristics
- A systemic autoimmune disease
- A chronic inflammatory disorder
- Attacks synovial joints (synovitis)
- Initially affects the small joints
- Genetic and environmental risk factors
- Affects 1% of the world population
- Women 3x more than men
- Onset often between 40-50 yrs
Rheumatoid Arthritis Co-morbidities
Co-morbidities;
- Skin (rheumatoid nodules)
- Lungs (fibrosis)
- Kidneys (amyloidosis)
- Heart (pericarditis, fibrosis, risk of MI)
- Blood vessels (atherosclerosis)
Rheumatoid Arthritis Overview
Rheumatoid arthritis (RA) is a chronic, systemic inflammatory disorder characterized by polyarthritis, progressive joint damage, immunologic abnormalities, and systemic inflammation. Its exact causes are unclear, but both genetic and environmental factors, such as infections and smoking, play a role. Only 15% of monozygotic twins show concordance, indicating significant environmental influence.
Activated autoreactive TH cells help B cells produce pathogenic autoantibodies, including rheumatoid factor (RF) and anti-citrullinated peptide antibodies (anti-CCP). RF is found in 70% of RA cases but also in other diseases, whereas anti-CCP is specific to RA. Autoantibodies can be present years before symptoms appear, and smoking increases RF occurrence and disease severity.
Cytokines drive the inflammatory response and immune dysfunction in RA, damaging target organs. The disease can affect other organs, leading to complications like rheumatoid nodules, lung fibrosis, kidney amyloidosis, heart issues (myocardial infarction, pericarditis, fibrosis), and atherosclerosis. These systemic effects may also result from RA therapy rather than the disease itself.
Common Autoantibodies to Neoantigens in RA
- Antibodies to IgG with defective glycosylation (rheumatoid factor, RF)
Self-associated IgG rheumatoid factors forming immune complexes
galactose - galactose pocket hypervariable combining site Fc epitope hypervariable combining site galactose pocket @ Elsevier. Male et al .: Immunology 7e - www .!
- Antibodies to citrullinated peptides
H O H O 1 N N peptidylarginine deiminase (PAD) 2+ Ca NH NH H,N+ NH2 0 NH2 L-arginine residue (+ charged) L-citrulline residue (neutral) Arthritis Research
RA Diagnosis and Autoantibody Role
- Early diagnosis of RA is crucial for effective treatment and preventing major joint damage. RA patients produce autoantibodies to various autoantigens years before symptoms appear, and RA can be transferred via antibodies. RF is present in about 75% of RA patients but also in other diseases and some healthy individuals. Despite its low specificity, RF is a common diagnostic marker for RA, measured by ELISA.
- RFs are antibodies targeting the Fc region of IgG and exist in every Ig class (IgG, IgM, IgA, IgE). IgG RF can form large immune complexes, further activating the immune system. Defective glycosylation of the Fc region enhances binding, creating stable, pro-inflammatory complexes that activate complement. Higher RF levels correlate with increased inflammation.
- The enzyme peptidylarginine deiminase (PADI) converts arginine to citrulline, crucial for the autogenicity of citrullinated proteins like synovial fibrin. Genetic polymorphisms in PADI4 may influence protein citrullination and antibody development. Smoking increases protein citrullination and specific antibody production. B-cells in the synovial fluid of anti-CCP positive RA patients produce anti-CCP antibodies, but circulating B-cells do not, indicating local citrullinated peptides drive CCP- specific B-cell maturation. Only RA patients develop antibodies to citrullinated synovial proteins, likely due to local inflammation and citrullinated peptide generation, such as during neutrophil NETosis.
T-cell Development and RA
- Normally; In the thymus, precursor thymocytes from the bone marrow initially develop as 'double-positive' cells expressing both CD4 and CD8, and low levels of the aß TCR. These undergo positive selection for weak, low affinity, interaction with self MHC class I or class II molecules on cortical epithelium, ie the cells are selected for their usefulness. Unselected cells (the majority) undergo programmed cell death by apoptosis.
- Cells undergoing positive selection lose one or the other of their co-receptor molecules (CD4 or CD8). Cells that interact with MHC class I on the thymic epithelium become CD8+ cells, and those that interact with MHC class II on the thymic epithelium become CD4+ cells.
- Finally, self-reactive cells that react strongly and with high affinity to self antigens presented on cells (dendritic cells and macrophages) in the thymus are eliminated by apoptosis (negative selection). The mature T-cell pool contains T-cells able to react to foreign proteins and also those that are able to react weakly to self antigens or react strongly to self antigens that they have not seen, for example antigens in peripheral tissues, including the joints.
- In RA; Genetic factors influence multiple pathways of antigen presentation to T-cells (input) and T-cell responses (output). The major genetic risk factor is in the HLA gene coding for MHC class II and is associated with the presence of autoantibodies.
- Defective positive and negative selection in the thymus are reported in models of RA. Defects in negative selection would bias the TCR repertoire towards autoreactivity. Defects in positive selection may cause lymphopenia (a decrease in the number of circulating T-cells), which has been shown to be a risk factor for autoimmunity.
- Lymphopenia due to a decreased output from the thymus is followed by a cycle of peripheral homeostatic proliferation, or self-replication, of naïve T-cells to restore T-cell numbers. This process of expansion in the periphery favours T-cells with autoreactive potential, ie those that recognise and have a higher affinity to self antigens and have lower threshold for activation. This increases the risk of developing inflammation in the synovium in RA.
TCR Repertoire and Selection
random expression of of TCR repertoire positive selection: exposure to MHC molecules negative selection: exposure to self antigen mature T cell pool precursor low αβ low aß high aß high «₿ 4+8+ 8+ no interaction with MHC class I + self peptide 8+ MHC class 1 MHC class | + self peptide 4+8+ 8+ cortical epithelium dendritic cells macrophages medullary epithelium TCR-induced cell death 4-8- 4=8+ 4+8+ 4+8+ 4+ MHC class Il + self peptide MHC class II 4+8+ 4+ no interaction with MHC class II + self peptide 4+ TCRs 4-8- no engagement with MHC programmed cell death C) Elsevier. Male et al .: Immunology 7e - www.studentconsult.com
Thymus and Peripheral T-cell Pool in RA
Thymus Reduced output Peripheral T-cell pool Increased self-replication 1 Peripheral T-cell selection T-cell immunosenescence
- clonal expansion
- contraction in diversity
- shift in gene expression and functional profile
- development of an autoimmune repertoire
RA TRENDS in Immunology
T-cell Dynamics in RA Development
- Individuals who develop RA go through a stage of accelerated self-replication of peripheral T cells, which compensates for a premature decline in thymic output, particularly in aged individuals. In most patients, RA occurs at the age of 40-50, several decades after formation of the T-cell repertoire has finished and thymic function is reduced or ceased.
- Peripheral T-cell homeostasis is maintained through positive selection and the replication of naïve T-cells that recognise self antigens. With peripheral selection being prominent, the T-cell repertoire loses diversity and is biased towards autoreactivity. The disease reflects a breakdown in tolerance to common antigens that are preferentially recognized in the synovium and clonal expansion of autoreactive T-cells. The best characterised autoimmune responses in patients RA are directed at neoantigens.
- Autoreactive T-cells entering the circulation develop into potent effector cells via a number of possible mechanisms. T-cell effector functions acquired with premature senescence are crucial in shaping the disease manifestations. For example, they lose expression of CD28 and become independent of co- stimulation pathways for activation and function. They have increased resistance to apoptosis, increased survival and cytotoxic abilities through perforins and granzymes (normally found in CD8 cells).
- Regulatory T-cells are a natural T-cell subset generated in the thymus, that regulate peripheral immune responses. Patients with RA have a deficiency in regulatory T-cell (Treg) function, and limited ability to suppress antigen presentation and T-cell activation through the immunosuppressive cytokines TGFß and IL-10. Depletion or functional degeneration of regulatory T-cells favours inflammatory responses.
Can’t find what you’re looking for?
Explore more topics in the Algor library or create your own materials with AI.
