Cancro al pancreas: anatomia, epidemiologia, fattori di rischio e terapia
Documento del Prof. Michele Reni sul cancro al pancreas. Il Pdf, utile per lo studio universitario di Biologia, esamina la complessità anatomica, l'epidemiologia, la prognosi, i fattori di rischio e le strategie terapeutiche, inclusi gli approcci chirurgici e chemioterapici.
Mostra di più11 pagine

Visualizza gratis il Pdf completo
Registrati per accedere all’intero documento e trasformarlo con l’AI.
Anteprima
Corso: Approccio chirurgico al paziente
Prof. Michele Reni Editor: Giorgia Mandanici 24/03/2025 Lecture nº1
Cancro al pancreas
Complessità anatomica del cancro al pancreas
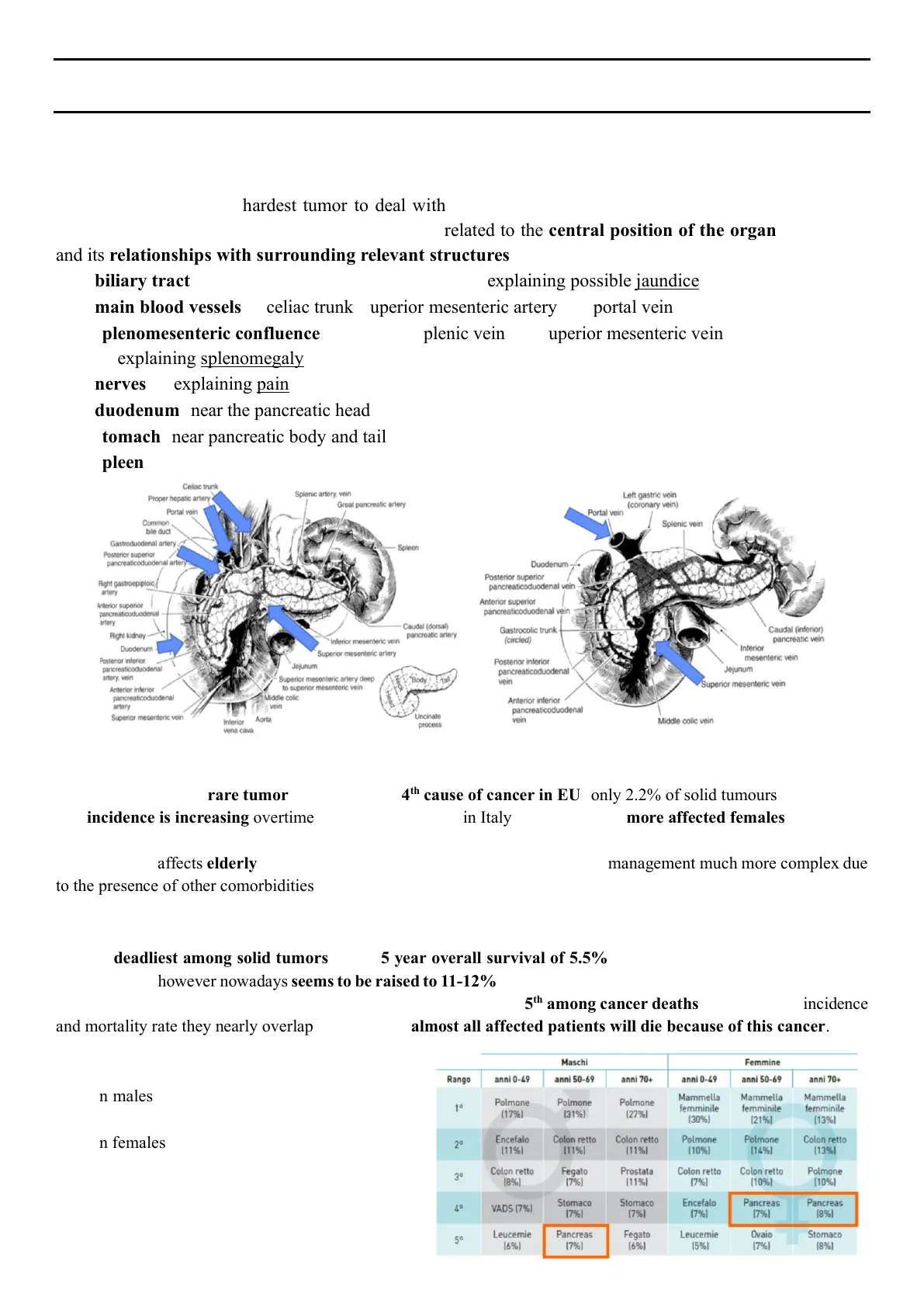
Pancreatic cancer is the hardest tumor to deal with in medical oncology for several reasons among which anatomical complexity is the most important one, related to the central position of the organ in the body and its relationships with surrounding relevant structures including:
- mainly head tumors
- biliary tract (common bile duct or choledochus) > explaining possible jaundice at diagnosis
- main blood vessels as celiac trunk, superior mesenteric artery and portal vein
- splenomesenteric confluence made up by splenic vein and superior mesenteric vein to form portal vein > explaining splenomegaly because of unproper blood flow towards these vessels
- nerves> explaining pain referred by patients perineural invasion
- duodenum (near the pancreatic head)
- stomach (near pancreatic body and tail)
- spleen
Celiac trunk Proper hepatic artery Portal vein Splenic artery, vein Great pancreatic artery Common bile duct Gastroduodenal artery Spleen Posterior superior pancreaticoduodenal artery Duodenum -. Posterior superior pancreaticoduodenal vein Right gastroepiploic, artery Anterior superior pancreaticoduodenal vein Anterior superior pancreaticoduodenal artery Caudal (dorsal) pancreatic artery Gastrocolic trunk (circled) Caudal (inferior) pancreatic vein Duodenum Inferior mesenteric vein Superior mesenteric artery Inferior mesenteric vein Posterior inferior pancreaticoduodenal artery, vein Jejunum Jejunum Superior mesenteric artery deep to superior mesenteric vein "Body Superior mesenteric vein Anterior inferior pancreaticoduodenal artery Middle colic vein Head Anterior inferior pancreaticoduodenal vein Middle colic vein
Epidemiologia del cancro al pancreas
Pancreatic cancer is a rare tumor ranking as the 14th cause of cancer in EU (only 2.2% of solid tumours). The incidence is increasing overtime > 15,000 new cases in Italy every year with more affected females than males compared to other countries (the reason of this epidemiological pattern is not known).but in general higher prevalence in males In particular it affects elderly - with a median age at diagnosis of 71- making its management much more complex due to the presence of other comorbidities that may also influence treatment decisions. most frequently diagnosed among people aged 65-74
Prognosi del cancro al pancreas
It is the deadliest among solid tumors with a 5 year overall survival of 5.5% (the lowest survival rate among solid tumors) which however nowadays seems to be raised to 11-12% (even if it varies based on which tumors are considered in the ranking). Despite being the 14th cause of cancer in EU, it is the 5th among cancer deaths > looking for incidence and mortality rate they nearly overlap meaning that almost all affected patients will die because of this cancer. Looking at these epidemiological data, in Italy:
- in males is the 5th leading cause of death in the age group 50-69
- in females is the 4th leading cause of death after the age of 50
Maschi Femmine Rango anni 0-49 anni 50-69 anni 70+ anni 0-49 anni 50-69 anni 70+ 1º Polmone (17%) Polmone (31%) Polmone [27%) Mammella femminile (30%) Mammella femminile (21%) Mammella femminile [13%) 2° Encefalo [11%) Colon retto [11%) Colon retto [11%) Polmone [10%) Polmone [14%] Colon retto [13%) 3º Colon retto (8%) Fegato (7%) Prostata [11%) Colon retto (7%) Colon retto [10%) Polmone [10%) 4º VADS (7%) Stomaco [7%] Stomaco (7%) Encefalo (7%) Pancreas (7%) Pancreas (8%) 5° Leucemie (6%) Pancreas (7%) Fegato [6%] Leucemie (5%) Ovaio (7%) Stomaco (8%)
Left gastric vein (coronary vein) Portal vein Splenic vein Superior mesenteric vein Aorta Inferior vena cava Uncinate process Posterior inferior pancreaticoduodenal vein Right kidney
Numeri stimati dal 2022 al 2050
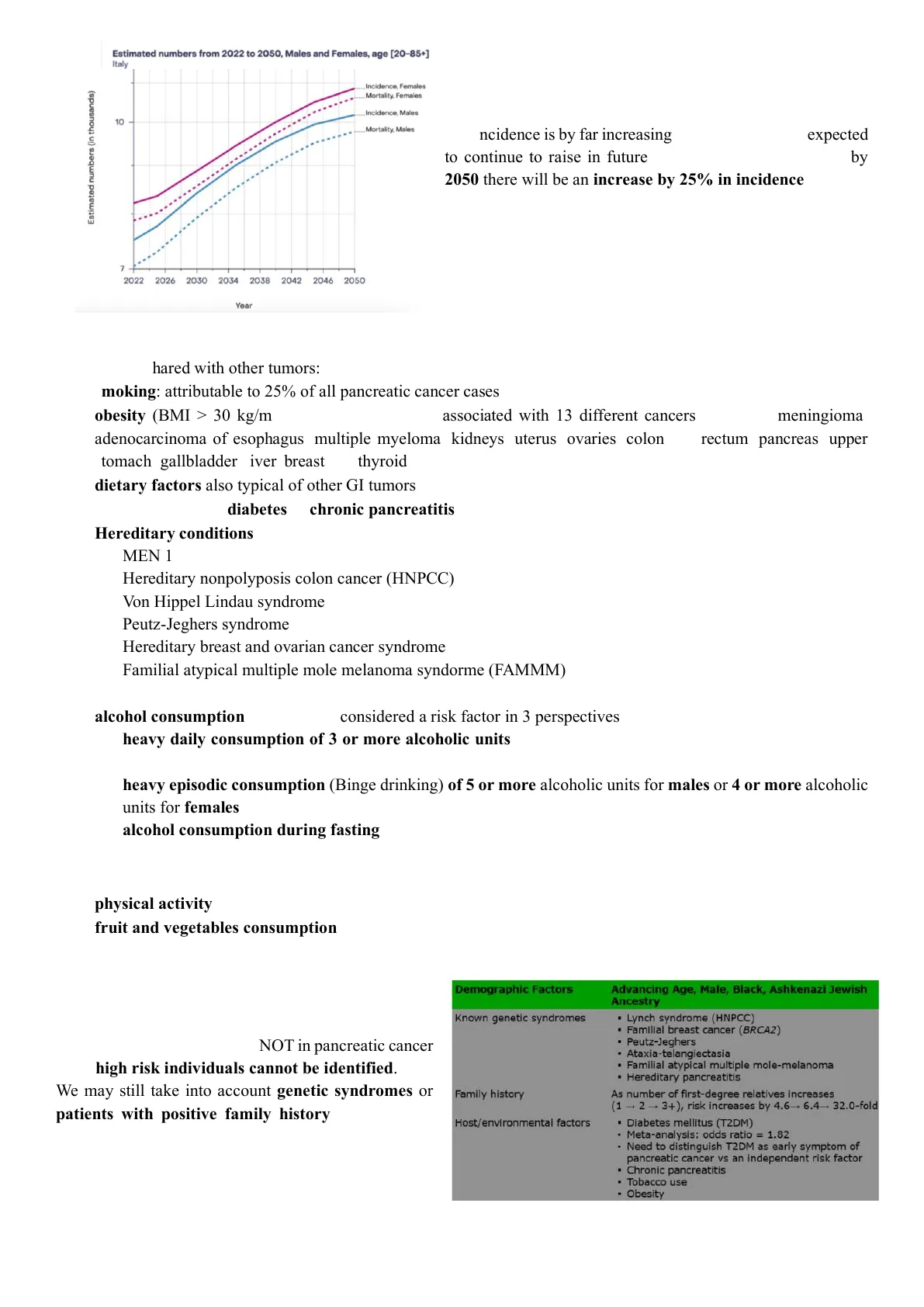
Estimated numbers from 2022 to 2050, Males and Females, age [20-85+] Italy Incidence, Females Mortality, Females Estimated numbers (in thousands) Incidence, Males 10 Mortality, Males 7 - 2022 2026 2030 2034 2038 2042 2046 2050 Year The incidence is by far increasing since 2022 and it is expected to continue to raise in future. This projection shows that by 2050 there will be an increase by 25% in incidence!
Fattori di rischio del cancro al pancreas
They are are shared with other tumors:
- smoking: attributable to 25% of all pancreatic cancer cases
- obesity (BMI > 30 kg/m2) it is known to be associated with 13 different cancers including: meningioma, adenocarcinoma of esophagus, multiple myeloma, kidneys, uterus, ovaries, colon and rectum, pancreas, upper stomach, gallbladder, liver, breast and thyroid
- dietary factors also typical of other GI tumors butter, saturated fat, red meat, processed foods, and low fruit and folate intake
- personal history of diabetes or chronic pancreatitis excessive alcohol consumption
- Hereditary conditions - MEN 1 syndrome pituitary tumor, parathyroid tumor, pancreas tumor: menin - Hereditary nonpolyposis colon cancer (HNPCC) aka Lynch Syndrome - Von Hippel Lindau syndrome - Peutz-Jeghers syndrome STK11 gene - Hereditary breast and ovarian cancer syndrome - Familial atypical multiple mole melanoma syndorme (FAMMM)
- Alcohol is classified by IARC(International Agency for Research on Cancer): group 1 alcohol consumption > should be considered a risk factor in 3 perspectives: - heavy daily consumption of 3 or more alcoholic units (1 alcoholic unit corresponds to 1 glass of wine or 330 ml of beer or 1 small glass of superalcoholic) - heavy episodic consumption (Binge drinking) of 5 or more alcoholic units for males or 4 or more alcoholic units for females - alcohol consumption during fasting
Fattori protettivi
- physical activity
- fruit and vegetables consumption > at best only 13% of people consume 5 portions of fruits and/or vegetables per day
Screening per il cancro al pancreas
It is useful for some cancers as breast, colon, prostate or gynecological tumors but it is NOT in pancreatic cancer since high risk individuals cannot be identified. We may still take into account genetic syndromes or patients with positive family history but when the follow up patients with genetic syndromes, they usually do not take into account pancreas since it is difficult to diagnose cancer at this level.
Fattori demografici
Advancing Age, Male, Black, Ashkenazi Jewish Ancestry
Sindromi genetiche note
- Lynch syndrome (HNPCC)
- Familial breast cancer (BRCA2)
- Peutz-Jeghers
- Ataxia-telangiectasia
- Familial atypical multiple mole-melanoma
- Hereditary pancreatitis
Anamnesi familiare
As number of first-degree relatives increases (1 - 2 - 3+), risk increases by 4.6-+ 6.4-+ 32.0-fold
Fattori ospite/ambientali
- Diabetes mellitus (T2DM)
- Meta-analysis: odds ratio = 1.82
- Need to distinguish T2DM as early symptom of pancreatic cancer vs an independent risk factor
- Chronic pancreatitis
- Tobacco use
- Obesity
Sfide diagnostiche del cancro al pancreas
Pancreatic cancer is difficult to diagnose for several reasons:
- Instruments are not so effective This manuscript (2015) from Marseille - one of the high volume centers in Europe for pancreatic cancer treatment- revealed that about 40% of their patients needed venous resection because of venous infiltration which was not predicted by preoperative CT scan highlighting that instruments are not sufficient and adequate to properly depict the relationship of the tumor with the great abdominal blood vessels. Also metastasis cannot be detected preoperatively or not be found since they appear later due to the presence of micrometastasis
- Experience of the radiologists is not always sufficient This study has been conducted in Netherlands by another high volume center for pancreatic cancer. In this case, 107 abdominal CT scans performed in other Dutch centers, for staging of locally advanced pancreatic cancer, have been reviewed and it has been found that 2 out of 3 had to be repeated due to unacceptable quality. Ann Surg Oncol (2015) 22:1874-1883 DOI 10.1245/s10434-014-4304-3 Annals of SURGICALONCOLOGY CrossMark OFFICIAL JOURNAL OF THE SOCIETY OF FUREACAL ONCOLOGY ORIGINAL ARTICLE - PANCREATIC TUMORS Pancreatic Adenocarcinoma with Venous Involvement: Is Up- Front Synchronous Portal-Superior Mesenteric Vein Resection Still Justified? A Survey of the Association Française de Chirurgie Jean Robert Delpero, MD', Jean Marie Boher, PhD2, Alain Sauvanet, MD3, Yves Patrice Le Treut, MD4, Antonio Sa-Cunha, MD5, Jean Yves Mabrut, MD", Laurence Chiche, MD', Olivier Turrini, MD', Philippe Bachellier, MD5, and François Paye, MDº and 323 (80 %) of 402 VR patients (p < 0.01). Venous wall was abnormal on preoperative CT in 266 patients who underwent planned VR, while 166 patients underwent VR without any previous suggestive CT findings. 41% Staging for locally advanced pancreatic cancer EJSO M.J.M. Morak ", J.J. Hermans b. H.G. Smeenk ", W.M. Renders ", J.J.M.E. Nuyuens , G. Kazemier ª, C.H.J. van Eijck ª# Results: After reviewing 107 abdominal CT scans from referral centres 73 (68%) scans had to be repeated due to unacceptable quality. Locally advanced disease was confirmed in 59 (55%) patients metastatic disease was found in 24 patients (22%). resect able disease was found in 6 patients, uncertain unresectable disease in 13 patients
- CT scan underestimates response to treatment especially after neoadjuvant therapy due to desmoplastic reaction of the tumor PET scan CT scan has some limitations, this is the reason why sometimes other instruments - as are needed. Micrometastasis and perineural invasion are undetectable on CT scan. Furthermore, inflammation can mimic vascular involvement 120 1.50 54mm 3mm 400.2 DV393.8 #:ID_STATION S.H. S RAFFAELE MILANO Mdc ?: CE D 415 HOST-95143 2mm Looking at the CT scans, no changes are observable at the site of pancreatic lesion after treatment and for this reason the disease is considered to be stable but if we look at the PET scan, the contrast enhancement seen at the beginning then disappears, suggesting complete metabolic response (despite the stable disease at CT).
Diagnosi tardiva del cancro al pancreas
At diagnosis, 60% of patients present with metastatic disease showing a median overall survival of just 11 months, indicating that diagnosis is often made at a late stage or that the tumor is quite aggressive from the beginning. Moreover, 30% of patients present with locally advanced disease (thus not resectable) with median overall survival of 19 months. In the remaining 10% of cases, patients have resectable tumors which are associated with 24 months of median overall survival.
Locally advanced: 30% Resectable: 10% Metastatic: 60%
Sopravvivenza globale mediana
Median OS (months) 10% Resectable: 24 months 30% Locally advanced: 19 months 60% Metastatic: 11 months
TOP images = before treatment > pancreatic lesion is observable surrounding the celiac trunk BOTTOM images = 2 months after therapy UNOO 3
Non hai trovato quello che cercavi?
Esplora altri argomenti nella Algor library o crea direttamente i tuoi materiali con l’AI.
